

INTRODUCTION
With colorectal cancer (CRC) being one of the most common malignancies encountered in the global population, its importance as a public health issue is acknowledged. According to WHO data, the incidence rate of the disease in 2020 was 1.9 million new cases worldwide, accounting for 10% of all newly diagnosed malignancies, making it the third most frequent cancer1. Regarding mortality rates, CRC was responsible for 9.4% of all cancer-caused deaths (a total of 9.96 million deaths), which makes it the third leading cause of cancer-related deaths in both genders worldwide1. In the same year in Greece, the incidence and mortality rate of CRC was 10.1% and 10.3% of all malignancies, respectively2.
Population screening for cancer prevention, when designed and funded effectively, can reduce the disease’s mortality and incidence rates3. Various methods used for CRC screening have appeared to be able to reduce mortality and the incidence rate of the disease as well, in cases where endoscopy was chosen4,5. CRC screening is more cost-effective compared to the absence of screening programs6. Based on current scientific research, Fecal Immunochemical Testing (FIT) showed increased participation, has been recommended as the first option for CRC screening, and has a low cost7.
In Europe, formal population-based screening programs that address all citizens aged 50–74 years are implemented in Finland, France, Slovenia and the UK. In most other countries, roll-out or opportunistically organized screening programs, result in sometimes major differences within one country, or within different age groups8. In Greece, CRC screening is opportunistic. Current CRC screening recommendations are based on a diagnostic protocol published by the Ministry of Health9. Greek recommendations apply to those aged 50–75 years and prioritize colonoscopy and FIT over other diagnostic tests. CT colonoscopy is considered a second-line examination, under special indications9. However, in a study that examined the implementation of recommendations by primary care professionals (PCPs), only 25% of them prescribed appropriate diagnostic tests10. Indeed, a second study on the use of colonoscopy in 11 European countries highlighted that Greece had the lowest compliance rate (8.2%) (95% CI: 6.7–9.2)11. An earlier study reported even lower compliance with fecal occult blood test (FOBT) (4.77%)12. One explanation for the low compliance with CRC screening recommendations may be the discrepancy between PCPs’ and healthy, unscreened citizens’ views about actual barriers to CRC screening, leading to inappropriate counseling by PCPs. It seems that the general population barriers for colonoscopy are lack of symptoms, negligence, and lack of PCP recommendation. PCPs were more likely to agree, for fear of the pain of colonoscopy, fear of cancer diagnosis, and embarrassment13.
The involvement of General Practitioners (GPs) in CRC screening is considered essential, as prevention is an important part of primary health care (PHC) services14,15. It also appears that GPs’ attitudes towards these tests in terms of screening interventions have an impact on their catchment population16. A systematic review on CRC screening awareness in European PHC argues that while the majority of GPs recommend screening tests for CRC, these are primarily aimed at high-risk patients17. Previous studies, examining GPs’ views regarding CRC screening, show that their attitudes appear to be influenced by their education, their ability to perform necessary tests as well as the characteristics of the population they treat18,19. Among the obstacles PCPs face in the implementation of cancer screening are the ambiguity of guidelines, lack of time, low acceptance by patients, insufficient patient information, preparation and complications of some of the tests, and cost of the necessary examination for the health system20,21.
The different perceptions and low rates of compliance with the CRC screening recommendations highlight the need for an in-depth study of the views of PCPs in Greece. The aim of this study is to highlight the views of GPs, regarding the obstacles encountered in Greece when promoting CRC screening, in order to reveal possible changes in the health system that will increase compliance.
METHODS
Study design and setting
In order to gain a better insight into PCPs’ views about CRC screening, a qualitative study was designed using semi-structured interviews. This was a multi-center study that included GPs from Central and Northern Greece (three out of the seven Regional Health Authorities) in order to include a variety of GPs that met the sampling purpose. The study protocol was initiated and designed by the Aristotle University of Thessaloniki Primary Health Care Research Network (AUTH.PHC.RN). The study protocol was approved by the 2nd, 3rd and 4th Regional Health Authorities of Greece.
Sampling and data collection
GPs members of the Educational and Research Network in PHC and GPs of AUTH Medical School working in different geographical regions in Central and Northern Greece were asked to recruit a prospective participant. Eighty-two of the invited GPs responded that they were interested in participating, and were informed, via email and telephone, about the study protocol. Αs gender, age, professional experience and the location of work structures may influence GPs’ views about CRC screening21-26, we proceeded with a purposive sampling strategy, intended to reach maximum variation of the sample. We aimed to recruit at least 10 males and 10 females; at least 10 with <10 years and 10 with ≥10 years working experience; at least 10 working at >30 km and 10 working at <10 km from screening facilities; at least 5 working in an urban, 5 in a semi-urban, 5 in a rural area, and 5 on an island; at least 10 working in the public sector and 5 working in the private sector.
An interview guide for the semi-structured interviews about CRC barriers was developed by the research team, based on existing literature18-21. The interview guide was pilot tested by three GPs to ensure clarity, and necessary adjustments were made. The final version is presented in Table 1.
Table 1
GPs’ interview topic guide on attitudes and beliefs on barriers of colorectal cancer screening in Greece, 2020
Fifty GPs, whose characteristics fulfilled the criteria of the study, were selected and recruited from March 2019 to January 2020. Thirty-two of them were finally included in the study and then the interviews stopped because the sample reached a point of saturation, as no new codes emerged from our analysis and all concepts in the theory were well-developed22. Telephone interviews with the participants were conducted by two researchers, with each interview lasting between 20 to 30 minutes.
Regarding the protection of research data, all the files were kept in electronic records, accessible only to certain research team members using strong passwords. The set of personal data was known only to a researcher responsible for its collection and maintenance. Only the necessary part of the personal data was known to the researchers who conducted the interviews in order to contact the participants. After this process, each participant was given a code that preserved their anonymity throughout the study. The researchers who performed the analysis and wrote the results and discussion did not have access to the participants’ personal data but only to their identification code.
Data analysis
The semi-structured interviews were recorded as an audio file and then transcribed verbatim by seven members of AUTH.PHC.RN. As well as conducting the interviews, the first transcripts were analyzed independently by two researchers and the results of the analysis were compared in order to discuss differences and reach an agreement between the categories of analysis. Data were processed and the six phases of thematic analysis according to Braun and Clarke23 were followed. This method allows the analysis of participants’ experiences in-depth and provides a wealth of content that cannot be recorded by a specific questionnaire.
Coding
As stated above, the principles of thematic analysis were followed. Firstly, the interviews were transcribed. Transcripts were carefully read many times by two independent researchers, in order to isolate material that was useful according to the research questions. The material was coded, giving the data a conceptual definition. Codes were identified according to the study’s aim. Then, repeated conceptual patterns were identified and categorized into themes. The procedure to conduct the thematic analysis and meet the trustworthiness criteria in this study was a reflective process moving back and forth during the six phases. An initial coding framework was applied to subsequent transcripts, and the addition of new or revised codes created the final format, which applied to all transcripts. The final analysis was agreed upon by the two researchers via discussion. At the end, the results were displayed. Each topic was presented in detail and separately to highlight its uniqueness. Thematic map, which emerged from the analysis, was also presented and connected the issues. Discussions among the AUTH.PHC. RN members about the findings were carried out, in order to increase the trustworthiness of the results and prevent interpretation bias.
RESULTS
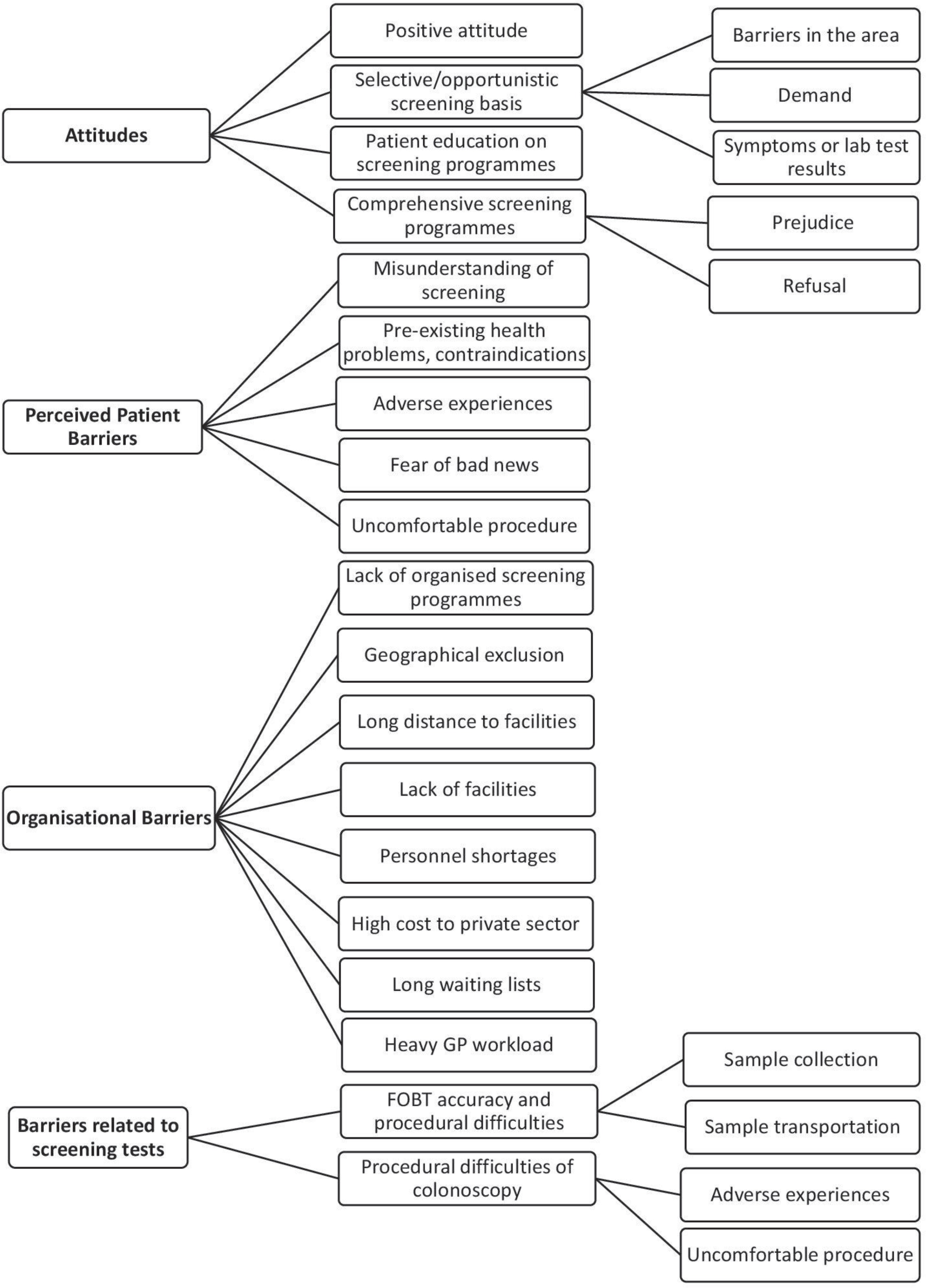
The participants’ main characteristics are given in Table 2. Thematic analysis generated the thematic map presented in Figure 1, regarding GPs’ attitudes and referring to the perceived barriers of CRC screening according to the study participants. The themes that emerged refer to: 1) GPs attitudes, 2) perceived patient barriers, 3) organizational and structural barriers, and 4) barriers related to screening tests.
Table 2
Descriptive characteristics of the GPs interviewed about colorectal cancer screening in Greece, 2020 (N=32)
Figure 1
Thematic analysis generated regarding GPs’ attitudes and referring to the perceived barriers of CRC screening according to the study participants
GPs’ attitudes
Generally, GPs reported that they have a positive attitude towards CRC screening, which is usually expressed as a recommendation to everyone fulfilling screening criteria and visiting the doctor’s office for any type of consultation or specifically for preventive services. Sometimes their positive attitude is expressed by only providing information about the need for colorectal screening:
‘I try to have every patient who is over 50 get a colonoscopy, and at the same time patients who are under 50 but have a family history of colon cancer, get screened earlier.’ (GP 1)
‘I will remind every patient aged over 50 years old at least once and definitely in any discussion for a preventive examination, that is what I always do when a patient comes and asks for an exam, a check-up, saying that in addition to the blood tests you do for lipids and blood sugar and so on and so forth, it is well known that it is very effective and correct to do a colonoscopy over 50.’ (GP 20)
Nevertheless, when analyzing answers to the question: ‘Can you describe the last time you had to recommend these screening tests to a patient?’, we concluded that there is selective prompting by some GPs, led by the presence of symptomatology or laboratory findings that indicate CRC:
‘Usually when there is diabetes from a very early age. When there is diabetes mellitus, obesity, and a sedentary lifestyle from a very early age, I start and suggest screening them after the age of 40, timidly.’ (GP 11)
Other reasons for referral are positive family history and comorbidity. GPs are less likely to recommend CRC screening in the presence of obstacles (which are presented in the following section). According to the results of this study, people consulting PHC clinics rarely request for CRC screening, unless there is a positive family history of colon cancer:
‘If someone tells me that a first-degree relative has had gastrointestinal cancer, I may still recommend a colonoscopy at 40. If someone tells me there is no such history and that they have no symptoms, I may not recommend it even at 60.’ (GP 7)
Perceived patient barriers
According to this study, GPs believe that their patients face obstacles in the process of CRC screening and are influenced by a number of factors (Figure 1). GPs claimed that there are people/patients who do not believe in the usefulness of screening or are embarrassed about exposing their bodies to health professionals, a problem that is more common in men and especially the elderly. Additionally, they believe that people’s perceptions are also affected by their own previous experiences or those of their relatives/friends, who have usually ‘suffered from’ a colonoscopy procedure and convey their negative experiences of this investigation. Moreover, GPs report that many patients decline to carry out CRC screening due to the fear of uncomfortable results:
‘Fear of the test itself, they are afraid that it will be painful, that they may be in pain, that it will have some complications ... it is perhaps more the fear of the test depending on what they may have heard from others … that it was painful...many may be ashamed ... it is a bit taboo ... Fear of the outcome, many patients are afraid of the test result and that it will turn out that they have a health problem.’ (GP 19)
Finally, pre-existing health problems, taking multiple medications, and aged >90 years may be contraindications to recommending colonoscopy in some patients:
‘Some of them are very old, have anatomical difficulties, i.e. kyphosis, or have many health problems, so it can be difficult to examine them.’ (GP 19)
Organizational and structural barriers
GPs reported many barriers due to a lack of available public health facilities and designated personnel (Figure 1). They pointed out that the main problem is the reduced capacity of gastroenterology specialists in public structures. According to their experience, there are large areas that have only one or no gastroenterologist working in the public sector and thus patients are eventually referred to private doctors. As a result, they say, there is a long waiting list for a colonoscopy mostly in the public, but also in the private sector. Access is often difficult on the mainland, but even more on the islands, where in some cases ‘geographical exclusion’ is mentioned. They mention that sometimes it is difficult to even access PHC units, especially in urban areas, due to the lack of public transportation.
‘The difficulty of finding the right structures. This is the problem we have in general. That is, when you advise a patient to have a colonoscopy, they say, “Yes, doctor, and when?”. My appointment is scheduled for after 6 months. And how am I going to get from my village to the city? There isn’t even a bus to pass through there. My kids must take me there and they can’t because they are working. These are everyday things that we encounter and so they say: “no it doesn’t matter, let me die ... let me not know what I have.’ (GP 4)
GPs participating in our study added that even where there is access, the increased workload and the insufficient knowledge of the CRC screening guidelines make it difficult for GPs to refer their patients for a colonoscopy:
‘In primary care, we have many patients with long-term health problems to manage and finding time to discuss screening is difficult. There’s not much time left to do it.’ (GP 2)
‘Everyone should know the guidelines … It is unthinkable that a GP does not know about the prevention of CRC. I consider the lack of this knowledge to be malpractice.’ (GP 22)
According to GPs’ views, even though colonoscopy is free of charge in the public sector, the above-mentioned obstacles render colonoscopy only possible in the private sector, where citizens are faced with another important obstacle; the cost of colonoscopy (to be paid by the patient), which is considerably increased when transport costs to screening facilities are also taken into account:
‘In times of economic crisis, telling the other person to go and have a colonoscopy for these reasons, but you will have to pay 100–150 euros ... Immediately creates an obstacle.’ (GP 2)
GPs’ perceived barriers about the screening tests
The participants mainly reported obstacles during the colonoscopy procedure (Figure 1). Colonoscopy, as an invasive procedure, usually causes discomfort, with difficulties starting from preparation and peaking in the implementation phase. On the other hand, participants stated that the FOBT has significant restrictions in the accuracy of results, but also some difficulties in the procedure (sampling and transferring samples for analysis):
‘The procedure (referring to colonoscopy) is a bit difficult, how to clean the intestine, the whole process, the diet, how to take the laxative, etc. … this and that makes it difficult for them, especially when they are older and it is difficult for them to understand how it should be done.’ (GP 13)
‘It’s more the nature of the test, like the FOBT, that creates some issues ... collecting the material and taking it for testing.’ (GP 31)
DISCUSSION
This study highlights the views of GPs in Greece regarding the barriers to CRC implementation, which can be taken into account for structural changes in the healthcare system, in order to increase compliance.
Barriers highlighted in this study relate to both the promotion and the implementation of CRC screening. Regarding CRC screening promotion, barriers were found similar to other screening methods, such as the lack of adequate knowledge on the prevention of CRC and the shortage of time during consultations to pass this knowledge on to the population14,21,24,25,27,28. According to our study, GPs mentioned that patients and doctors are facing obstacles both in the existing screening procedures and also in the insufficient logistical infrastructure of the national health system in their effort to implement CRC screening.
Our data show that GPs generally recognize the value of screening for CRC, as they suggest existing prevention methods in appropriate age groups. However, some of them have not yet consolidated the preventive nature of the examination. As a result, they are hesitant to propose it to asymptomatic individuals. Similar concerns are emerging from studies in other countries19,21. Still, there is confusion in distinguishing primary from secondary prevention for CRC, as the study lists modifiable risk factors, such as obesity, sedentary lifestyle and comorbidity (diabetes mellitus) as reasons for secondary instead of primary prevention. The issue of inadequate continuous medical education on the prevention of CRC is therefore being raised in the international medical community14,21,24,25. This is an important obstacle to screening fortification, as studies conducted in countries where screening for CRC is largely applied have shown that population participation is influenced by the knowledge of PCPs on how to prevent this disease and their ability to explain the need for screening21,25.
In order to reinforce prevention as a belief in people and increase their compliance with screening, it is necessary for GPs to devote time to communicate its necessity and benefits based on patients’ wishes and capabilities26. At the same time, the involvement of doctors in mainly administrative procedures, such as recurrent prescribing, and also in the management of chronic diseases of their patients, as our study showed, leaves little time for prevention and screening, an issue that is also recorded in studies abroad21,27,28.
The present study highlighted that the promotion of CRC screening is also influenced by GPs’ beliefs about the obstacles posed by their patients. These might reflect the views of patients, yet they are inwardly shaped by the beliefs and experiences of doctors themselves, as showcased in literature13,20,25. Most of the prejudices that emerge both in these and in international studies are related to colonoscopy. Many relate to the fear of an unpleasant outcome, the lack of information about the existence of CRC prevention methods and unfortunately, the inability to understand the usefulness of screening, especially by older males15,29. Studies show that women, perhaps because of their involvement in other secondary prevention programs, such as breast or cervical cancer, understand the value of preventing this disease and are more engaged18,30. Educating the public on these issues would be a valuable task performed by GPs and PCPs. Systematic health education by doctors on the feasibility and benefits of CRC screening, which is also the wish of the patients themselves, will aid in overcoming the above-mentioned obstacles14,15,25,31.
This study showed, in line with other international studies32-34, a variety of important barriers to the use of colonoscopy. The invasive nature of this method, its high cost, and the strong resistance of patients, as perceived by doctors, to have it performed in the absence of symptoms, leads many physicians to suggest it selectively to patients, especially in high-risk ones due to positive family history, aiming at diagnosing the disease. This phenomenon is also recorded in the international literature21 and may be the main barrier to the use of colonoscopy for prevention.
Apart from the attitudes and opinions of GPs, structural and operational problems of the Hellenic Health System raise additional obstacles to the implementation of CRC screening. Despite the establishment of a protocol for the prevention of CRC by the Ministry of Health9 and contrary to international studies recording the use of state directives in increasing compliance with prevention programs19,27, our study showed that this is unfortunately not followed; screening is carried out opportunistically and based on individual initiative, either that of the physician or the patient. Focusing on the views of the GPs involved in the study, the manpower and the existing logistical infrastructure in both the public and private sectors cannot, at this stage, support the massive implementation of the screening protocol. Participants identified that deficiencies in hemoglobin detection reagents in feces are often reported, while a colonoscopy in public health structures can take months to be scheduled, due to the distance of these structures from the person’s place of residence combined with the cost of travel. Regarding the private sector, GPs note that the cost of colonoscopy is high and mostly borne by the insured, as also shown in the international literature28,35. In addition, referring individuals from a public to a private structure can be considered directed and raises transparency issues. As a result of the above-mentioned obstacles, GPs often come to a dead end, unable to direct the patient in either the public or the private sector.
Despite the proven value of CRC screening, the present study has highlighted a number of obstacles that make its implementation difficult. This situation is reflected in international studies, with the barriers reported being similar in both developing and developed countries25.
Limitations
When interpreting the results, methodological limitations must be considered. Despite the saturation of views in this study, there is always the possibility that unexpressed views exist. Furthermore, data based only on perceptions of GPs and not on other health professionals working in PHC or even in the population, can be biased towards a more medically-centered perspective. Studies investigating attitudes and barriers from the perspectives of citizens are needed to contribute to a more comprehensive understanding of the inadequate CRC screening implementation in Greece.
CONCLUSIONS
Summarizing the findings of this study in Greece, GPs generally recognize the value of screening for CRC and highlight barriers to screening that are multifactorial. These include deficiencies in the health system, difficulties related to the patient and difficulties related to the examination process. The combination of improving the knowledge of GPs with the aim of increasing public awareness of the value of prevention, as well as the implementation of structural and operational changes in the Hellenic Health System, may facilitate the overcoming of important obstacles to the effective implementation of CRC screening. These improvements are particularly important in non-urban areas of the country, where access to CRC screening services is much rarer and more difficult.