
INTRODUCTION
Immunization through vaccination is a proven strategy to protect public health from severe and sometimes fatal infectious diseases such as diphtheria, tetanus, pertussis, tuberculosis, polio, measles, and hepatitis B, including respiratory infections such as influenza1-3. Comprehensive implementation of vaccination programs has substantially reduced the morbidity of these diseases and contributed to reducing health disparities within and across the globe4. However, the efforts have not achieved universal coverage due to unequal access to vaccines and fluctuations in public confidence in their efficacy and safety, resulting in deaths from vaccine-preventable diseases in European countries5.
The World Health Organization’s Strategic Advisory Group of Experts on Immunization (SAGE) define vaccine hesitancy as ‘delay in acceptance or refusal of vaccine despite the availability of vaccine services … which in turn is influenced by factors such as complacency, convenience, and confidence’, known as the 3Cs model6. While complacency and convenience are driven by the perceived risk of disease and accessibility of vaccine services, confidence is related to beliefs and understanding of the effectiveness and safety of vaccines and trust towards the healthcare system. Although high confidence in vaccination programs is crucial for maintaining high coverage rates, in 2016, a 67-country survey conducted by the Vaccine Confidence Project (VCP) found that the European region had lower confidence in the safety of vaccines than other world regions7. Furthermore, the European Commission concluded in its 2018 report that the overall state of confidence in vaccine safety and effectiveness in Europe was an area of further concern8. At the same time, a systematic review of published European evidence did conclude that individuals have many safety concerns about vaccination and often believe that the risks of vaccination outweigh its benefits9.
Knowledge is necessary, although not sufficient, element to promote vaccination. As described by the Health Belief Model10, beliefs about benefits and risks of getting or not getting a vaccination are vital components to encourage vaccination as a personal health-seeking behavior, and these beliefs are determined by multiple factors such as demographic variables, psychosocial factors, and personality traits, including health knowledge. In light of the above, the objective of this study is to provide an insight on the level of knowledge of vaccination, the predictors of correct or incorrect knowledge about vaccines, and examine the associations between the level of knowledge and vaccination uptake among adults and children in 28 European countries.
METHODS
Data source
This secondary dataset analysis was performed on publicly available de-identified data. Data were obtained from the Special Eurobarometer 488 on Europeans’ attitudes towards vaccination, collected on behalf of the European Commission, Directorate-General for Health and Food Safety (DG SANTE) during 15–29 March 2019 across 28 European Countries, before Brexit. The full report and complete information on the methodological approach of this survey, including contact rates, are available elsewhere11. Participants from different demographic groups were interviewed face-to-face at home in their first language. The data consisted of approximately 1000 respondents aged ≥15 years per country. Two exceptional countries had a smaller sample size (n=512 for Luxembourg, and n=497 for Malta), leading to a pooled sample size of 27524 adults. Data were post-stratified by sex, age, region NUTS II (basic regions as defined by the EUROSTAT nomenclature of territorial units for statistics), and size of locality. A comparison was made between the sample composition and population distributions of each participating country to adjust for non-response.
Measures
Knowledge score and index
Knowledge about vaccination within the Eurobarometer survey was assessed with the following four true/false questions: ‘For each of the following statements, could you please tell me whether you think it is true or false. 1) vaccines overload and weaken the immune system; 2) vaccines can cause the disease against which they protect; 3) vaccines can often produce serious side-effects; and 4) vaccines are rigorously tested before being authorized for use’. The correct answers were false, false, false, and true. We assessed respondents’ knowledge as a score by summing up the number of questions respondents provided a correct answer (range: 0–4). The knowledge score was further classified for analysis purposes into low knowledge (0–2 correct responses) and high knowledge (3–4 correct responses).
Vaccination in the past five years for respondents themselves and children
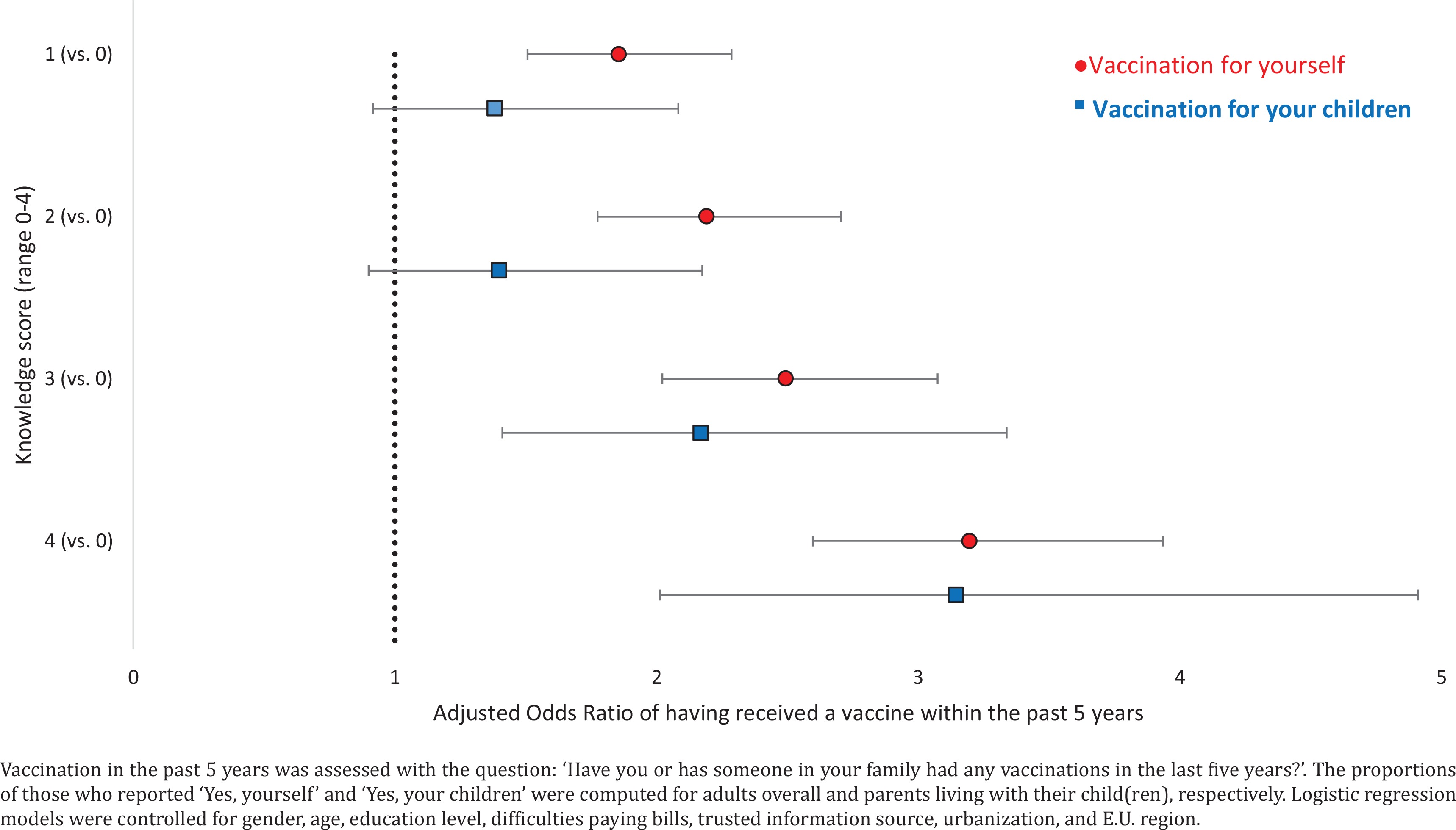
Vaccination in the past five years was assessed with the question: ‘Have you or has someone in your family had any vaccinations in the last five years?’. The proportions of those who reported ‘Yes, yourself’ and ‘Yes, your children’ were computed for adults overall and parents living with their child(ren), respectively.
Sociodemographic characteristics
The following sociodemographic characteristics were assessed: country, gender, age, education level, difficulty in paying bills (as a proxy of socioeconomic status), most trusted source of information, urbanization, E.U. region, parental status, perceived effectiveness of vaccination, and vaccination in the past five years. Education was assessed as the respondents’ age when they stopped full-time education with the question: ‘How old were you when you stopped full-time education?’. Socioeconomic status was assessed with a proxy question related to the difficulty in paying bills with the question: ‘During the last twelve months, how often have you had difficulties in paying bills at the end of the month…?’. Within the context of this database, parents were defined as respondents who lived with their children aged 0–14 years (as defined by the Eurobarometer). Perceived effectiveness of vaccination was assessed by asking whether respondents thought that ‘vaccines can be effective in preventing infectious diseases such as flu, measles, polio, hepatitis, meningitis, and tetanus’.
Statistical analysis
Data were weighted to be nationally representative of each of the participating countries. Descriptive statistics were computed for the 28 European Countries overall and by country with 95% Confidence Intervals (CIs). T-tests were used to examine differences in mean knowledge score with statistical significance set at p<0.05. To investigate associations between a higher level of knowledge (3–4) and vaccination in the past five years, multivariable logistic regression models were fitted separately for two denominators: respondents overall, and those who lived with a child aged 0–14 years (n=6005), leading to the reporting of adjusted odds ratios (AOR) and their 95% Cis, controlling for gender, age, education, difficulties paying bills, most trusted source of information, urbanization, and E.U. region. Logistic regression analysis was also used to examine predictors of knowledge levels. All analyses were conducted with R version 3.6.2.
RESULTS
Mean knowledge score
Out of the maximum obtainable score of 4, the mean knowledge score among adults overall in the 28 European countries was 2.2 (95% CI: 2.2–2.3), with little variation noted by gender and age (Table 1). At the national level, the mean knowledge score ranged from 1.7 in Bulgaria (95% CI: 1.6–1.8) and Cyprus (95% CI: 1.6–1.8), to 3.0 in the Netherlands (95% CI: 2.9–3.0) and Sweden (95% CI: 2.9–3.1). While knowledge scores did not differ significantly by gender for most of the countries, women had a higher mean score in Austria (2.3 vs 2.1), and men had a higher mean score in Finland (2.6 vs 2.4), France (2.2 vs 1.9), and Slovenia (2.0 vs 1.8).
Table 1
Mean knowledge score among adults in 28 European countries, Special Eurobarometer 488, 2019 (N=27524)
[i] Estimates were weighted to address non-response. Knowledge score was assessed as sum of the respondents’ correct answers to the following 4 questions: ‘For each of the following statements, could you please tell me whether you think it is true or false: 1) vaccines overload and weaken the immune system; 2) vaccines can cause the disease against which they protect; 3) vaccines can often produce serious side-effects; and 4) vaccines are rigorously tested before being authorized for use’. Differences in mean knowledge score were tested by t-test (p<0.05, bold).
Percentages and predictors of high knowledge
Among adults overall, 46.3% (95% CI: 45.2–47.3) were classified as having a higher level of knowledge about vaccination (knowledge score 3–4), as seen in Table 2. Significant variations were seen by education level, with the lowest percentage among adults that had no full-time education (27.9%, 95% CI: 18.8–37.1) and the highest among those who finished full-time education at ≥20 years old (54.4%, 95% CI: 52.6–56.2). The percentage of adults with a higher knowledge score was lower among those who reported difficulties paying bills most of the time (31.3%, 95% CI: 27.8–34.7), followed by those who reported difficulties from time to time (41.1%, 95% CI: 39.0–43.3), and higher among those reported difficulties almost never/never (50.2%, 95% CI: 48.9–51.5). With regard to the most trusted source of information on vaccination, lower percentages of high knowledge were seen for those who did not provide specific answers (don’t know/none/other) (24.8%, 95% CI: 20.2–29.5) followed by those who reported the internet (33.8%, 95% CI: 28.0–39.6); the highest percentage was observed among those who reported health authorities as the trusted source of information (58.2%, 95% CI: 55.2–61.2). By region, the lowest percentage of the population with higher scores in knowledge was seen in Eastern Europe (42.6%, 95% CI: 40.9–44.3). In comparison, the highest percentage of the population with an increased knowledge score was seen in Northern Europe (50.3%, 95% CI: 47.4–53.3).
Table 2
Percentages and predictors of high knowledge about vaccination among adults in 28 European countries, Special Eurobarometer 488, 2019 (N=27524)
After adjusting for all the sociodemographic characteristics assessed, associations between sociodemographic characteristics and high knowledge had a similar pattern to that observed at the bivariate level. The odds of having a higher level of knowledge about vaccination were higher among respondents with a higher educational level. Moreover, those who did not report difficulty in paying bills were more likely to have a higher knowledge score (AOR=1.73; 95% CI: 1.43–2.09) when compared to those who had difficulties most of the time. Respondents who trusted most the health authorities as a source of information were more likely to have high knowledge about vaccination (AOR=1.29; 95% CI: 1.12–1.50), while those who reported the internet as their most trusted source of information (AOR=0.71; 95% C.I: 0.53–0.94) were less likely to have a high knowledge score when compared to those that reported healthcare providers as their most trusted source. Those who lived in large towns were more likely to have high knowledge about vaccination (AOR=1.22; 95% CI: 1.08–1.37) than those in rural villages.
Associations between knowledge and vaccination for adults and children
Among adults overall, previous vaccination among respondents themselves in the past five years increased with a higher knowledge score as noted in Figure 1. Compared to those who scored 0, the odds of vaccination were 1.86 (95% CI: 1.51–2.29), 2.19 (95% CI: 1.77–2.71), 2.49 (95% CI: 2.02–3.07), and 3.20 (95% CI: 2.60–3.94) times higher among those who scored 1/4, 2/4, 3/4, and 4/4, respectively. Similarly, among adults living with their children, the odds of vaccination for their children were significantly higher among those who scored 3/4 (AOR=2.17; 95% CI: 1.41–3.34) and those who scored 4/4 (AOR=3.15; 95% CI: 2.01–4.91) than those who scored 0, indicating that the level of correct knowledge on vaccinations is associated with increased vaccination among adults and children in Europe.
DISCUSSION
Our study revealed significant variations in knowledge about vaccination across 28 European countries. While high knowledge was not predicted by demographic characteristics such as gender, age, region, or presence of a child, it showed significant associations with respondents’ educational level, socioeconomic status, and urbanization, with higher knowledge scores reported among those of more advantaged socioeconomic status. Furthermore, a dose-response association was observed between increasing knowledge of vaccinations and an increased likelihood of immunization in the past 5 years for adults and their children, respectively.
Previous research performed by the European Commission has noted that generally, across the 28 E.U. countries, public perceptions towards vaccines are primarily positive. The majority of adults in the E.U. agree that vaccines are important, safe, effective, and compatible with religious beliefs8. In line with the above, in our secondary analysis of the 2019 Eurobarometer, we also observed a strong association between the perceived effectiveness of vaccination and having a higher knowledge score about immunization. Those who perceived vaccines to be effective were more likely to have higher knowledge scores than adults that noted vaccination to be probably effective.
Healthcare providers play an essential role in increasing knowledge of vaccines and promoting vaccination in their population. The 2018 European Commission report on vaccination noted a correlation between general practitioner (GP) confidence and confidence in vaccination among the general public in the survey: countries whose GPs hold higher confidence in vaccines tended to have a larger proportion of the public expressing positive vaccination beliefs8. Regional evidence has indicated inadequate vaccination rates and misconceptions among GPs that should be the focus of future evidence-based interferences with the potential to improve vaccination coverage of GPs significantly and indirectly of their patients12. Recent data collected during the COVID-19 pandemic among healthcare professionals before the outbreak, revealed that knowledge on vaccination was significantly associated with both attitudes and application in clinical practice, proposing that providers with high knowledge scores may have a more positive perception to preventive measures and stronger willingness to endorse preventive instructions13.
Europeans are increasingly exposed to health information via social media and the internet; it is essential to ensure that the correct information is easy to identify, access and understand14. In our multivariable analysis, a significant association was observed between the source of information that respondents most trust and having a higher knowledge about vaccination. Respondents who most trusted social networks or other websites to obtain information about vaccination were less likely to have higher levels of knowledge about vaccines. Previous studies have indicated an independent negative association between information about vaccine safety from the mass media and the likelihood of vaccination against HPV15. Potential explanations for this include both the availability and quality of information regarding vaccination in online resources and the health literacy of the users. Given the roles that the internet can play in health communication, it is important to disseminate valid and evidence-based information through multiple channels, including social media and other online sites to reach all populations, especially people with lower socioeconomic status and subpopulations which may have anti-vaccination attitudes16. While we identified higher SES to be associated with higher knowledge scores in principle, this may not reflect knowledge towards all vaccines. Although our results concur with the conclusions of a recent systematic review on child immunization in developed countries that indicated the existence of barriers to vaccination, especially among low SES children in several settings but for specific vaccines (MMR), low uptake might also be noted in other SES strata9.
While our analysis indicated the importance of knowledge about vaccination as a proxy of having performed a vaccination in the past 5 years although imperative to initiate contemplation, it is not the only defining factor for behavioral change. Self-efficacy also influences all aspects of behavior, including the attainment of new behaving modus and this appears as a major determining factor of one’s decision to perform or not a specific behavior by adapting motivation, thought processes and behavioral standards17. This is of specific interest in light of the COVID-19 vaccination that has been initiated across the globe, as previous research has indicated that factors such as previous vaccination for influenza and believing in the efficacy of COVID-19 vaccination has been found to increase the probability of accepting COVID-19 vaccination as soon as possible18,19.
Limitations
Our study is subject to several limitations. First, due to the cross-sectional nature of the survey, we were unable to establish causal relationships. Second, the responses were self-reported and subject to recall bias and social desirability bias. Third, the Eurobarometer only included four questions related to the knowledge of vaccines and hence may not have captured all related domains, while true/false questions used to assess respondents’ knowledge contained possibly subjective language such as ‘often’ and ‘rigorously’: this might have affected respondents’ answer choices. Lastly, the definition of parents used in this study might have resulted in the exclusion of parents who did not live with their children in the same household or inclusion of respondents who lived with their younger siblings or grandchildren under 15 years old. Despite the above, the large sample size and the geographical coverage of the Eurobarometer survey provide a robust dataset for the extrapolation of results that have direct relevance to the European Region, although the results represent the status quo prior to the COVID-19 pandemic.
CONCLUSIONS
Level of knowledge about vaccination varied significantly across the EU MS. Higher socioeconomic, higher educational level, and the perceived effectiveness of vaccination were significantly associated with higher levels of correct knowledge of vaccinations. Furthermore, the knowledge of vaccinations strongly was associated with previous vaccination among adults and reported for their children. Public health campaigns that educate adults about the efficacy of vaccination are warranted to help reduce disparities in knowledge that were noted across the EU MS and promote vaccination at the national and subnational levels20,21. Messages should be tailored to reach all populations, especially those with lower socioeconomic and educational level. These findings may be of specific interest to policymakers in light of the roll out of COVID-19 booster vaccinations across Europe.