

INTRODUCTION
The COVID-19 pandemic has had a significant impact on mental health of the general population, but due to certain factors, more so on healthcare professionals1,2. Due to the large number of infections, many healthcare professionals were forced to leave their departments and assist those working in the infectious wards. As a result, healthcare institutions had to deal with an increase in the number of necessary services, particularly in intensive care. The high stress levels were present due to work intensity, infrastructural and family challenges, provoking complex emotional responses that could have adversely affected individual and collective mental health3,4.
Depression5 and higher levels of anxiety and emotional distress6-8 were manifested as well. There were few studies that explored the gender differences on mental health problems during pandemic in health workers. Other studies, have found significant levels of mental health problems in health workers, with females at higher risk for depression, anxiety, post-traumatic stress disorder, and wellbeing9,10.
Among factors that were found to lessen adverse effects on mental health among health workers, emotional intelligence showed consistent results throughout different contexts11. Emotional intelligence is the ability to process and use information related to one’s and others’ emotions to direct behavior12. Studies show that individuals with high emotional intelligence, are able to adjust their emotions over time13 to successfully manage stress13, repair mood14, lower somatization15, and have a positive impact on mental health overall16.
Regarding the relationship between mental health problems and emotional intelligence, there is a gap in the literature comparing health workers, workers of other professions and non-workers, more so in collectivist cultures with underdeveloped medical systems such as in Kosova. The current study aims to evaluate the relationship between mental health externalizing and internalizing problems, stress in the workplace, gender and working status in association with emotional intelligence, during the COVID-19 pandemic in Kosova. The study will use the transactional model of stress to explicate the impact of emotional intelligence on mental health and somatization.
METHODS
Participants and procedure
Participants of this cross-sectional study were Albanian active students in their third year of nursing studies at the AAB College in Prishtina, Kosova. In total, 408 students were included in the study, 76% of them being female (n=310). We have included all the students from the nursing faculty without work-related interruptions. All the students who have been in the educational process have expressed their willingness to participate in the research. All participants gave their oral consent after it was clarified that their data would remain confidential. Their voluntary participation and their right not to participate were clarified. The data were provided through their ID code in order for the data not to be identified by name. Ten students of psychology were trained for the procedures of gathering the data. The procedures proposed complied with the Helsinki Declaration of 1975, as revised in 2008.
The convenience method of sampling was utilized. The average age for all participants was 27.17 years (SD=17.09). There were no statistically significant gender differences in the mean age distribution [MF=26.25, SDF=16.37; MM=30.07, SDM=18.97; t(408)= -1.96, p=0.075]. Most of the participants were living in urban areas (64.2%) and unmarried (73%). At the time of the survey, 25.5 % (n=104) of participants were unemployed, and 42.6% (n=174) had other non-health occupations. Among those working in the health sector, 2.9% (n=12) worked in the COVID-19 ward, 6.4 (n=26) in the general hospital, 4.9% (n=20) in intensive care unit, 5.1% (n=21) in emergency units and 12.5% (n=51) in primary care. In terms of being infected with COVID-19, 30.6% (n=125) were at some point in the past infected, 32.8% (n=134) were not, and 36.5% (n=149) did not know if they were infected or not.
Instruments
Adult Self-Report Questionnaire
The Adult Self-Report questionnaire was used to assess internalization and externalization problems. ASR (18-59) is a self-report instrument widely used to assess mental health problems in the adult population. ASR has been translated into various languages, including Albanian17. The ASR questionnaire assesses participants on what they have experienced in the last 6 months and takes 25–40 minutes to fill in.
Participants used a Likert scale with three levels: 0 = not true, 1 = somewhat or sometimes true, 2 = very true or often true, to respond to 134 items. This scale contains two subscales: 1) Internalizing problems (the sum of the points in the anxiety-depression, withdrawal, and somatic complaints; and 2) Externalizing problems (the sum of thought and attention problems, aggressive, rule-breaking and intrusive behavior). The third broad-spectrum scale is total problems, the sum of all the items on the form. For all degrees of the problem, a higher score represents a higher severity. In our sample, the ASR manifested excellent internal consistency: Cronbach’s α=0.968 for the total sample, and α=0.966 for males and α=0.969 for females.
Trait Emotional Intelligence Questionnaire-Short Form
The Trait Emotional Intelligence Questionnaire-Short Form (TEIQue-SF)18 is a 30-point self-report questionnaire, which takes 20 minutes and assesses the global emotional intelligence (EI) trait, as well as the four EI trait factors: welfare, self-control, emotionality, and sociability. The questionnaire was translated into Albanian (after permission from the Psychometric Laboratory, University College London) by three students of the English language faculty and the translation was discussed in a group of three, two psychologists and one linguist. The questionnaire was then piloted in 30 students and the comments that arose during the piloting were taken into consideration. Participants responded to the articles using a 7-point Likert scale ranging from 1 (strongly disagree or strongly disagree) to 7 (strongly agree or strongly agree). Cronbach’s for the total sample was good (α=0.844).
Stress Questionnaire
The Stress Questionnaire (SQ) assesses five stress-related factors, such as psychosocial working variables related to work-related stress, on a Likert scale ranging from 1 (absolutely agree) to 5 (absolutely disagree). It specifically assesses: 1) conflict roles, 2) support colleagues or collaboration, 3) supervisors’ support, 4) job requirements, and 5) work control. Overall, it takes up to 15 minutes to be administered. The questionnaire gives a total score ranging from 0 to 36, in which a higher score indicates a greater degree of psychological distress.
The first versions of the SQ were based on the Karasek19 demand, control and support model and the Health and Safety Executive’s Management Standards work-related stress20, and further developed adding emerging stress determinants such as the fear of crisis and non-employability21. The scale is easily understood by occupational physicians and quickly administered.
RESULTS
Prevalence analysis
This study has found the prevalence of internalizing and externalizing problems to be 14.9%. Specifically, internalization problems have shown a prevalence of 16.2%, and externalization of 14.9%. On the other hand, 9.8% of the participants have shown very low levels of emotional intelligence. Lastly, almost half of the participants reported high levels of stress (41.9%).
Emotional intelligence
Through analysis of independent between-groups ANOVA, statistical differences were found dependent on working status for all subscales of TEIQue-SF and total TEIQue-SF [F(2; 405)=48.84, p<0.001, η2=0.194 for total TEIQue-SF; F(2; 405)=45.48, p<0.001, η2=0.183 for well-being; F(2; 405)=31.67, p<0.001, η2=0.135 for self-control; F(2; 405)=25.08, p<0.001, η2=0.110 for emotionality; and F(2; 405)=16.20, p<0.001, η2=0.074 for sociability]. To evaluate the nature of the difference between the three means, a Fisher LSD post hoc test was used. A significant difference for the total TEIQue-SF scores between health workers and two other groups (non-health workers and without jobs) was observed [t(232)=7.53, p<0.001]. Further calculations are given in the Supplementary file.
Mental health
Gender differences were observed for the total ASR score, with females showing higher values (mean=40.33, SD=31.04) than males (mean=31.38, SD= 6.65) (Table 1). The Levene test of variance has shown that the difference between groups was statistically significant [t(406)= -2.57, p<0.01]. In terms of subscales, significant differences between groups were found on the internalizing problems subscale [t(406)= -3.90, p<0.001], with females reporting higher values.
Table 1
The relationship between internalizing, externalizing and total ASR with gender, residence, employment status, and infection status (N=408)
Regarding the status of working (health workers, non-health workers, and non-working), the independent between-groups ANOVA yielded a statistically significant effect [F(2; 405)=8.97, p<0.001, η2=0.04 for total ASR; F(2; 405)=45.48, p<0.001, η2=0.07 for internalizing problems; and F(2; 405)=31.67, p=0.006, η2= 00.03 for externalizing problems] (Table 1). To evaluate the nature of the difference between three means, a Fisher LSD post hoc test was used. The difference between health workers (mean=9.01, SD=97.34) and non-health workers group (mean=16.25, SD=13.27) was statistically significant [F(2; 405)=15.17, p<0.001] for total ASR. In both subscales, internalizing and externalizing problems, health workers have shown statistically significant lower means differences compared to non-health workers and those not working.
A one-way multivariate analysis of variance (MANOVA) test was performed to observe the interaction effects between profession, residence with internalizing, externalizing, and total ASR. Non-health workers were at high risk for emotional and behavioral problems on three broad scales (p<0.01). Participants from rural regions have shown a higher risk only for internalizing problems compared to those living in urban regions (p=0.04). There was no interaction effect between profession and residence.
Mental health and emotional intelligence
MANOVA was conducted to test the hypothesis that there would be a mean difference between level of emotional intelligence and ASR scores. A statistically significant MANOVA effect was found [Pillais’Trace=0.180, F(2; 405)=8.57, p<0.001, η2= 0.06] (Figure 1).
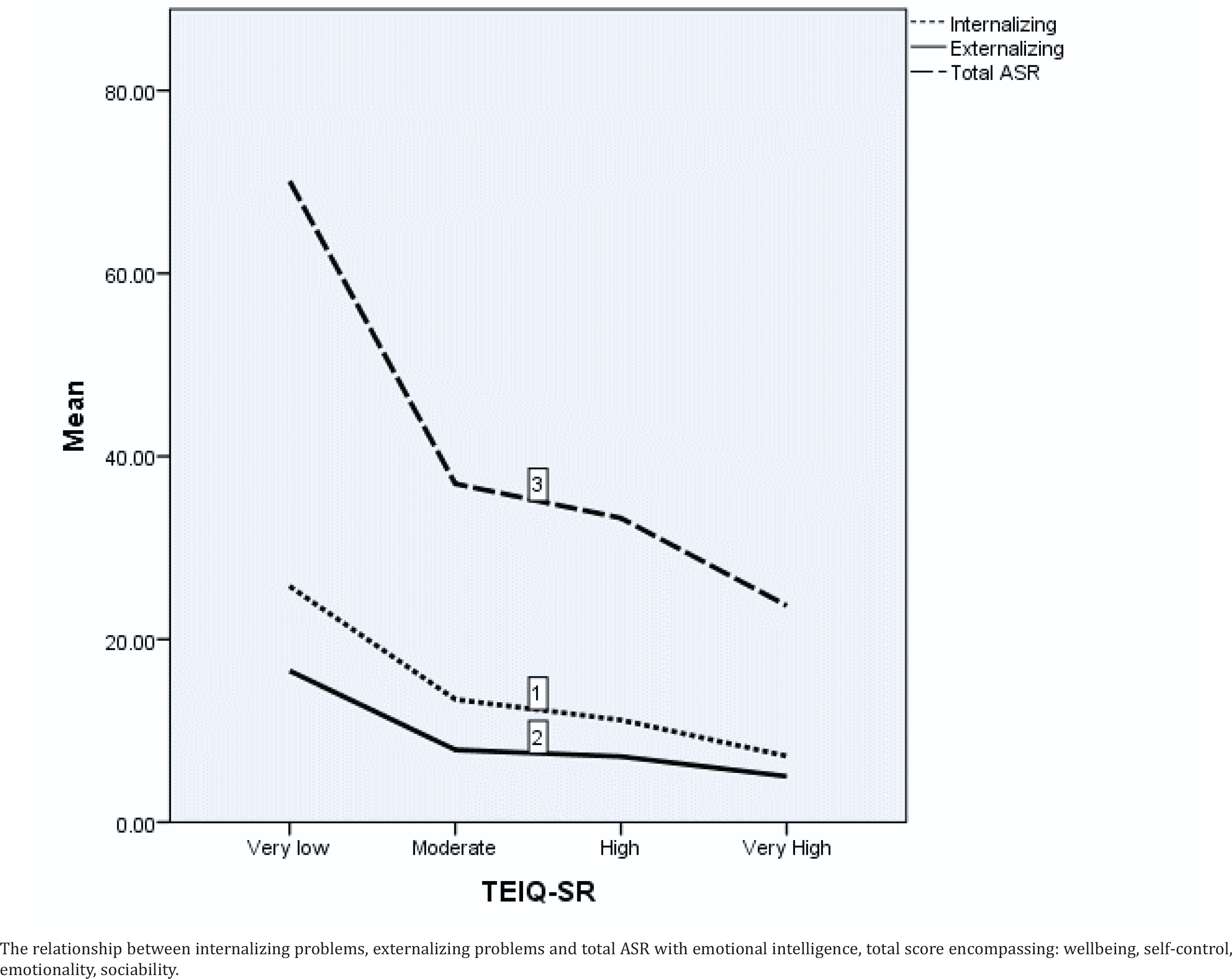
A series of post-hoc analyses (Fisher’s LSD) revealed a negative association between all four levels of emotional intelligence and all three broad scales of ASR. In the internalizing problem scale, externalizing problems scale and total scale, participants with high emotional intelligence had lower means compared to those with very low and moderate emotional intelligence. There were statistically significant mean differences between those with ‘very high’ and ‘very low’ emotional intelligence.
We found a significant interaction effect between TEIQue-SF and stress in the workplace scale with total ASR [F(3; 408)=1.75, p=0.155], with internalizing [F(3; 408)=2.01, p=0.112], and externalizing [F(3; 408)=2.05, p=0.106]. Participants with very high level of stress and very low emotional intelligence had higher scores in internalizing scale. The same results were found for externalizing and total scores. There was no interaction effect between TEIQue-SF, stress categories and place of work (4×4×3) with ASR scales.
Cluster K analysis
A cluster K analysis was performed to set up homogenous groups on the pattern of presenting mental health problems and stress-related to work. Data were clustered into four groups (both mental health problems (MHP) and high stress (13.7%; n=56); only MHP (26.5%; n=108); only stress (24%; n=98), and the group without any (35.8%, n=146). A chi-squared analysis 3×4 crossable was used for cluster groups and three categories of working status (not working at all, health workers, non-health workers). We used adjusted p-values (Bonferroni method) to test the differences between groups. The study found a significant relationship between proportion distributions of cluster groups according to working profile [χ2(6)=22.24, p<0.001].
In the health workers group, there were significant differences between health workers with both MHP and stress (2%) compared to only stress (10%) and group without MHP or stress (13.7%). The results showed that the highest risk group for both mental health problems and only mental health problems were participants in non-health professions.
MANOVA was also conducted to test if there would be one or more mean differences between cluster groups and emotional intelligence for total scale and subscales scores. A statistically significant MANOVA effect was obtained [Pillais’ Trace=0.14, F(3, 408)=3.91, p<0.001]. The multivariate effect size was estimated at 0.113, which implies that 11.3% of the variance of emotional intelligence was explained by cluster type. A series of one-way ANOVA on each of the four subscales of emotional intelligence was conducted as follow-up tests to the MANOVA. Results showed that all of the ANOVA were statistically significant, with effect sizes (partial ranging from a low of η2=0.027 (wellbeing) to a high of η2=0.08 (self-control). Participants from the first cluster group with mental health and stress had a significant higher risk for low level of emotional intelligence compare to other cluster groups.
DISCUSSION
This study aimed to explore the intricate relationship between mental health, emotional intelligence, internalizing and externalizing problems, workplace stress and demographic factors such as job status and gender. The study encompassed health workers, non-health workers and unemployed individuals. Gender impact was present at internalizing problems. Occupational status was associated with mental health, whereas health workers displayed less internalizing and externalizing problems compared to non-health workers and the unemployed. Emotional intelligence, in line with our predictions, was negatively associated with stress, internalizing and externalizing problems. Health workers had the highest results in all four subscales of emotional intelligence.
Overall, the study unraveled complex relationships between emotional intelligence, workplace stress, and mental health, emphasizing the protective role of emotional intelligence, especially in high-stress environments such as healthcare units during the pandemic. It also highlighted the influence of social support and the intriguing interaction between emotional intelligence and stress on mental health outcomes. Moreover, it challenged traditional gender stereotypes by showing no significant gender differences in emotional intelligence within this specific context.
Working in a medical setting during the pandemic could be among the most stressful jobs, exposing healthcare professionals to a high risk of anxiety and depression and other mental health difficulties22. Not corroborating other findings, we found the lowest levels of mental health difficulties were among health workers, in comparison to non-health workers and the unemployed. We assume that the social support and high scores on emotional intelligence of healthcare workers could have served as protective factors against mental health complications.
In other settings, high levels of social support helped health workers maintain their mental health by endowing them with the agility and strength to deal with unexpected situations, such as large fluxes of patients23. In China social support could significantly decrease mental health problems during the pandemic among health workers24, whereas in Germany, high levels of social support and optimism were among the strongest protective factors against depression and anxiety25.
Individuals with high emotional intelligence demonstrate greater emotional clarity11 and are able to regulate and manage their negative emotions positively26, which helps them preserve meaning in stressful situations27 and experience less psychological distress, especially in times like a global pandemic. Health workers with high emotional intelligence are usually more sensitive to the needs of others, which, in return, could enhance their ability to cope with emotional job demands and enhance the provision of patient care28.
Emotional intelligence may be useful as a moderator against workplace stressors and psychological health outcomes for health workers, by considerably increasing a sense of wellbeing at the workplace29. The personal and social skills that lead to superior performance at the workplace are mostly related to the emotional competence, encompassing emotional intelligence as an important construct in various areas of everyday life for both genders, including mental health, social functioning, and especially job performance and job satisfaction in the workplace30.
Other studies found that the ability to recognize and manage internal emotional states had the highest negative correlation with anxiety and internalization31 by helping doctors better prepare for stressful situations32, such as facing large numbers of patients in short intervals, developing more effective emotional strategies to face stressful situations, and avoiding being overwhelmed by them33. Furthermore, there is evidence that high scores on emotional intelligence dimensions can help with general health, including mental and physical health34. This relationship holds true for both general and clinical populations.
Our findings revealed that there is no significant difference between the mean scores of men and women on the emotional intelligence scale, unlike some previously reported findings where females had higher scores than males35, but corroborating others that did not find a gender effect on emotional intelligence36. We associate the lack of such effect in this study due to the heterogeneity of the participants who were in the same occupational profile and academic level.
Limitations
In the current study, it is important to acknowledge several limitations that may influence the interpretation of our findings. Firstly, our analyses were based on data collected from a sample of students who were concurrently engaged in both employment and academic studies. This dual role may introduce a potential confounding factor, as stressors could emanate from both work and educational commitments. Consequently, it is plausible that the observed effects on mental health outcomes, may differ from those experienced by healthcare professionals who are not simultaneously pursuing academic studies.
Secondly, we utilized self-report questionnaires to assess mental health symptoms. While these instruments are widely employed for their efficiency, they are inherently subject to biases that can lead to either an overestimation or underestimation of mental health issues. Employing clinical interviews alongside self-report measures, could provide a more comprehensive understanding of the mental health landscape, offering a clearer delineation of specific mental health pathologies related to emotional intelligence.
Moreover, our reliance on quantitative methods, while valuable for statistical analysis, may potentially provide a limited perspective on the complex relationship between emotional intelligence and mental health problems. To address this limitation, it is advisable to undertake further investigations using a mixed-methods approach. By integrating qualitative data collection methods, such as interviews or focus groups, alongside quantitative assessments, we can gain deeper insights into the nuanced protective role of emotional intelligence in the context of mental health.
In conclusion, while our study offers valuable insights into the association between emotional intelligence and mental health among students with dual roles, it is imperative to recognize these limitations. Future research endeavors should aim to incorporate clinical interviews, mixed-methods approaches, and larger and more diverse participant samples, to provide a more comprehensive and nuanced understanding of this critical topic.
CONCLUSIONS
The study found a relationship between mental health problems, emotional intelligence and stress at workplace. Health workers demonstrated higher scores in emotional intelligence and reported fewer mental health problems compared to non-health workers and the unemployed. Additionally, emotional intelligence was found to be negatively associated with mental health complications among health workers during the COVID-19 pandemic.
The study also suggests that emotional intelligence could be useful as a moderator against workplace stressors as well as internalizing and externalizing problems. Therefore, it is recommended that organizations provide training and support to enhance emotional intelligence skills among their employees, especially those in high-stress occupations such as healthcare. Of greater importance is the finding of the protective nature of emotional intelligence in times of crisis such as pandemics.