

INTRODUCTION
Nonprescription medicine and first-aid knowledge are increasingly critical areas for school health teachers. Recently, children have become vulnerable to various serious health problems while attending school because of the significant amount of time they spend there. These problems include unintentional injury, interpersonal violence, and both communicable and noncommunicable diseases1. Among these, unintentional injuries pose a particularly grave health threat to school-aged children because they can result in lifelong disabilities or even fatalities2.
The most common types of unintentional injuries and risks by children include falls, pedestrian and bicycling accidents, drowning, poisoning, fire-related burns, and suffocation, with the most of the injuries being preventable3. These injuries can occur at any time during the day, necessitating the provision of immediate lifesaving care or first aid to minimize the consequences of injuries4. In the literature, the term first aid tends to be used to refer to immediate assistance provided to an injured or sick person until professional help arrives, with the goal of preserving life, alleviating suffering, preventing further injury, and promoting recovery5. The prompt administration of first aid by school health teachers can minimize the morbidity and mortality of children attributed to injury-related problems, underscoring the importance of ensuring that the teachers possess adequate knowledge in this regard6,7.
Moreover, children may also experience health complications or unexpected illnesses while at school, with an increasing number of students requiring various levels of care for specialized health needs. Throughout the school year, children may require nonprescription medicines for acute illnesses, emergencies, or immediate pain relief8. As such, the preparedness of schools to respond to these emergencies and provide immediate access to emergency medication is critical9. Providing school health teachers with relevant information regarding the use of medication is a crucial component of any country’s overall healthcare delivery system, as these individuals can help ensure the rational use of medicines by conveying information to children, parents, and the community. However, regulations and guidelines governing medication administration at schools vary considerably around the world.
Although the responsibility for administering medication to children at school should ideally rest with healthcare professionals, such as school nurses10, the presence of full-time school nurses is limited in Thailand. However, in accordance with the requirements, each school is required to designate a minimum of one school health teacher along with multiple school health (student) leaders11. These individuals should undergo training specific to their respective roles and responsibilities prior to taking them on. Consequently, there is a need for nonprescription medication and first aid to be administered by school health teachers and auxiliary staff, many of whom have limited experience in providing school health services because of inadequate training12,13.
Despite the potential importance of nonprescription medication and first-aid knowledge among school health teachers, there remains a paucity of evidence about such factors and their associated determinants in Northern Thailand. In addition, there have been no studies that assessed the knowledge of nonprescription medication and first aid in Phayao Province, an area characterized by its rural setting with limited human resources, first-aid facilities, and access to basic medicines. This study therefore assessed the knowledge of nonprescription medicine and first aid, and the associated factors, among school health teachers in the province. The results of this study could be used to inform appropriate interventions and modifications to the school health teacher training curriculum, potentially leading to the development of new policies concerning children’s care in schools by local policymakers.
METHODS
Study design and setting
From June to August 2022, a cross-sectional study was carried out in Phayao Province, which is located approximately 700 km from Bangkok, the capital of Thailand. The study specifically targeted 216 public primary schools situated within nine districts of Phayao Province, all falling under the jurisdiction of the Phayao Province Administration Education Office.
Sample size calculation
Due to the dearth of published literature examining the knowledge pertaining to nonprescription medicine and first aid among primary school health teachers in Thailand, as well as within the designated study area, this study endeavored to ascertain the maximum feasible sample size. To accomplish this, a proportion of 50% (p=0.5) was carefully considered with the aim of obtaining the maximum possible sample size. This calculation resulted in a required sample size of 136, conducted at a 95% confidence level, with a margin of error set at 5.5%. Additionally, a 10% non-response rate among participants was incorporated to prevent the loss of the sample or incomplete data. Consequently, the study included a sample of 136 primary school health teachers, with each school appointing a single representative selected through purposive sampling techniques. To ensure the representativeness of the sample, samples were derived from primary schools covering each district where they were situated.
Study tool and variables
The self-administered questionnaire developed and created by the researchers was based on a survey of relevant literature and similar studies14,15. The questionnaire was evaluated for content validity using the index of item-objective congruence (IOC) of three experts in the fields of community nursing, school nursing, and community pharmacy, to ascertain completeness. The validity of the questionnaire as per the experts was calculated and found to have an IOC >0.5. A three-part questionnaire in the Thai language was utilized to gather data for this study. The first part included questions about the participant’s demographic characteristics, including gender, age, education level, whether possessing a degree related to health sciences, years of experience in teaching, years of experience in school health services, previous nonprescription medicine training, previous first-aid training, number of teaching hours per week, and school health service period. The selection of these specific factors was based on previous studies4,7,13,14,16-25. The second part of the instrument included 30 questions on nonprescription medicine knowledge. The participants were tested to determine whether their responses were true or false (a correct answer was scored as one point and an incorrect answer as zero). The total possible score ranged 0–30, with higher scores indicating higher knowledge of nonprescription medicine. Then, Bloom’s cut-off score26 was used to classify the knowledge into three levels. The participants who scored ≤60% were categorized as having a low level (score ≤18), 61–80% as having a moderate level (score 19–24), and >80% as having a high level (score ≥25). The observed Kuder–Richardson Formula 2027 (based on the 30 items) in our pilot study with 20 school health teachers (who were not included in the main study) was 0.81, suggesting a high level of internal consistency. The final part of the instrument included 20 questions on first-aid knowledge. The respondents were also tested to determine whether their responses were true or false (a correct answer was scored as one point and an incorrect answer as zero). The total possible score ranged 0–20. Higher scores indicated greater knowledge of first aid. Consequently, the calculated total scores based on Bloom’s cut-off score26 were also used to classify the knowledge into three levels. The participants who scored ≤60% were categorized as having a low level (score ≤12), 61–80% as having a moderate level (score 13–16), and >80% as having a high level (score ≥17). The observed Kuder–Richardson Formula 2027 (based on the 20 items) in our pilot study was 0.74, suggesting a high level of internal consistency.
Data collection
Official letters were secured to seek permission from both the Phayao Province administration’s education office and the selected schools. Prior to data collection, each participant was contacted and engaged through a personal visitation process lasting 1–2 weeks, for which appointments were made in advance. Permission to conduct the study was explicitly obtained from each participating school. Written informed consent was obtained from all participants after providing a comprehensive explanation of the study’s nature and objectives. Emphasis was placed on maintaining the confidentiality and anonymity of all individuals involved in the study throughout its duration.
The selection process for the study utilized the purposive sampling method to choose only one head school health teacher from each primary school. In cases where a selected head school health teacher declined to participate, a replacement from the same school was chosen to ensure the representation of the target group in the study. The inclusion criteria for participant selection were as follows: the teachers had to be currently employed in schools in Phayao, working as full-time teachers, possessing a minimum of one year of teaching experience, and expressing willingness to take part in the study. Upon obtaining the participants’ consent, the questionnaire was provided to them in a private and comfortable setting. It was emphasized that they should refrain from using communication tools or devices to search for information regarding nonprescription medicine and first aid. Participants were then requested to promptly return the completed questionnaire to the researcher.
Statistical analysis
Data collected from the study were organized and analyzed using IBM SPSS Statistics software version 29.0 (SPSS Inc., Chicago, Illinois, USA). Cronbach’s alpha coefficients were calculated to establish reliability. Demographic characteristics, nonprescription medicine knowledge levels, and first-aid knowledge levels were analyzed using descriptive statistics. The factors associated with knowledge scores of nonprescription medicines and first aid were examined using univariate analysis. Additionally, simple linear regression was undertaken to identify predictors of the knowledge scores of nonprescription medicines and first aid, and variables with a p<0.15 were then entered into the multiple linear regression model. Using the Enter method, statistically significant variables at the 0.05 level were entered into the final model. A variance inflation factor (VIF) value of <5 indicated the absence of multicollinearity28.
RESULTS
The study included a total of 134 primary school health teachers, resulting in an exceptional response rate of 98.5%. Among the participants, the majority (92.5%) were identified as female. The mean age of the participants was 42.5 ± 10.4 years, with 27.6% falling within the age groups of 31–40 and ≥51 years. The age of the respondents varied from 24 to 60 years. In terms of education level, the majority of the participants (70.9%) held Bachelor’s degrees, while 27.6% possessed postgraduate degrees, and the remaining participants had diplomas. It is worth noting that the vast majority (97.8%) of the participants did not possess any degree specifically related to the health sciences (Table 1).
Table 1
Sociodemographic characteristics of the school health teachers
Regarding professional experience, the mean duration of teaching experience was 15.9 ± 10.9 years. Among the participants, 41.8% had been working as teachers for a period of ≤10 years. Furthermore, the mean duration of experience in school health services was found to be 4.9 ± 6.0 years, with 41.8% of the participants having worked in this field for 2–5 years. It is noteworthy that a large proportion of school health teachers (73.9%) reported having received previous training in nonprescription medicine, whereas 59.7% had undergone prior first-aid training. In terms of weekly workload, the mean number of teaching hours per week was 20.6 ± 7.1 hours. Slightly over half of the participants (55.2%) reported having a teaching load of ≥21 hours per week (Table 1).
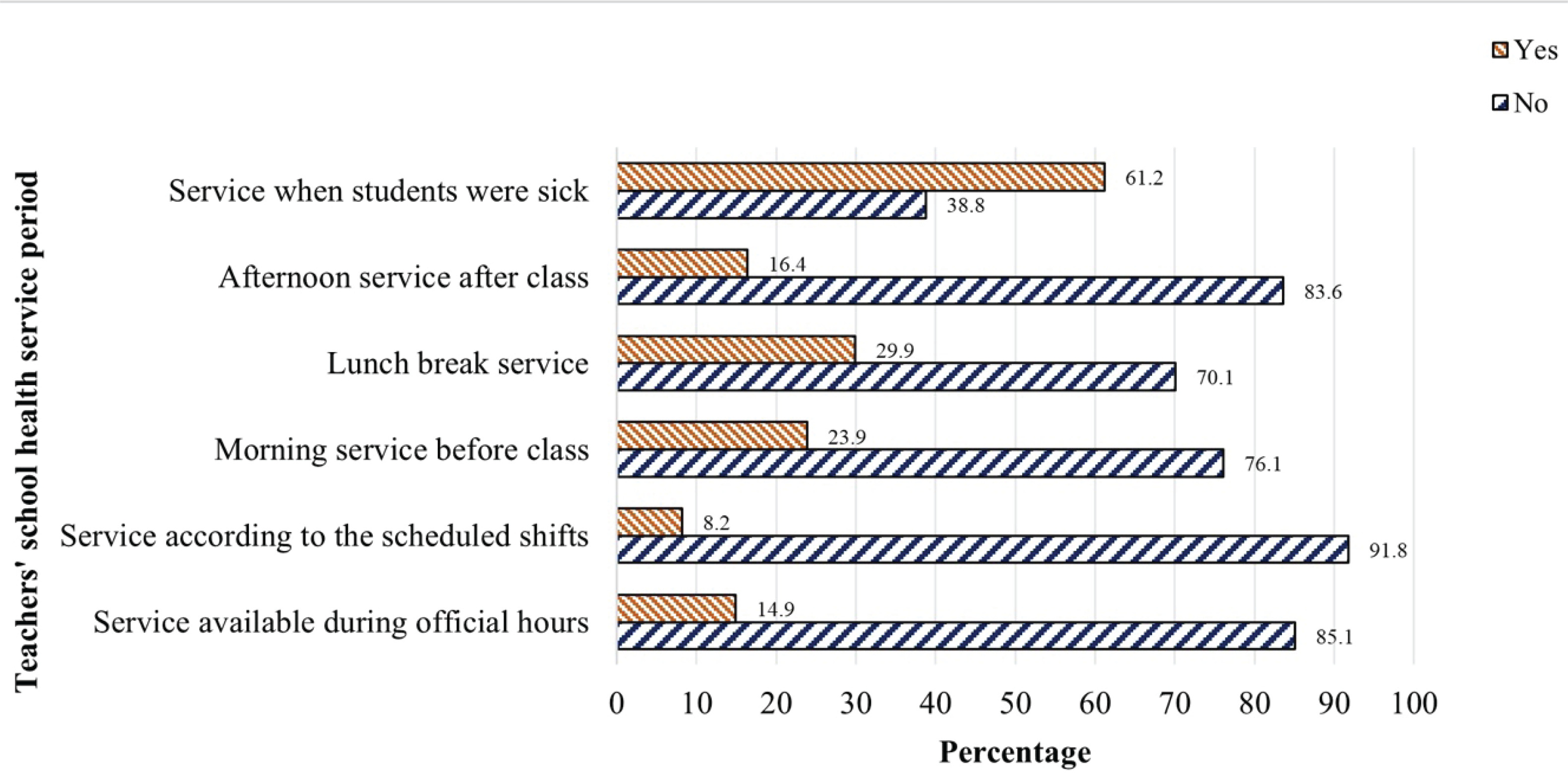
The majority of the participants (61.2%) provided health services when students were sick, 29.9% offered services during lunch breaks, and 23.9% were available only in the morning service before class. Only 8.2% provided service according to the scheduled shifts or aligned with the assigned schedule for each health teacher (Figure 1).
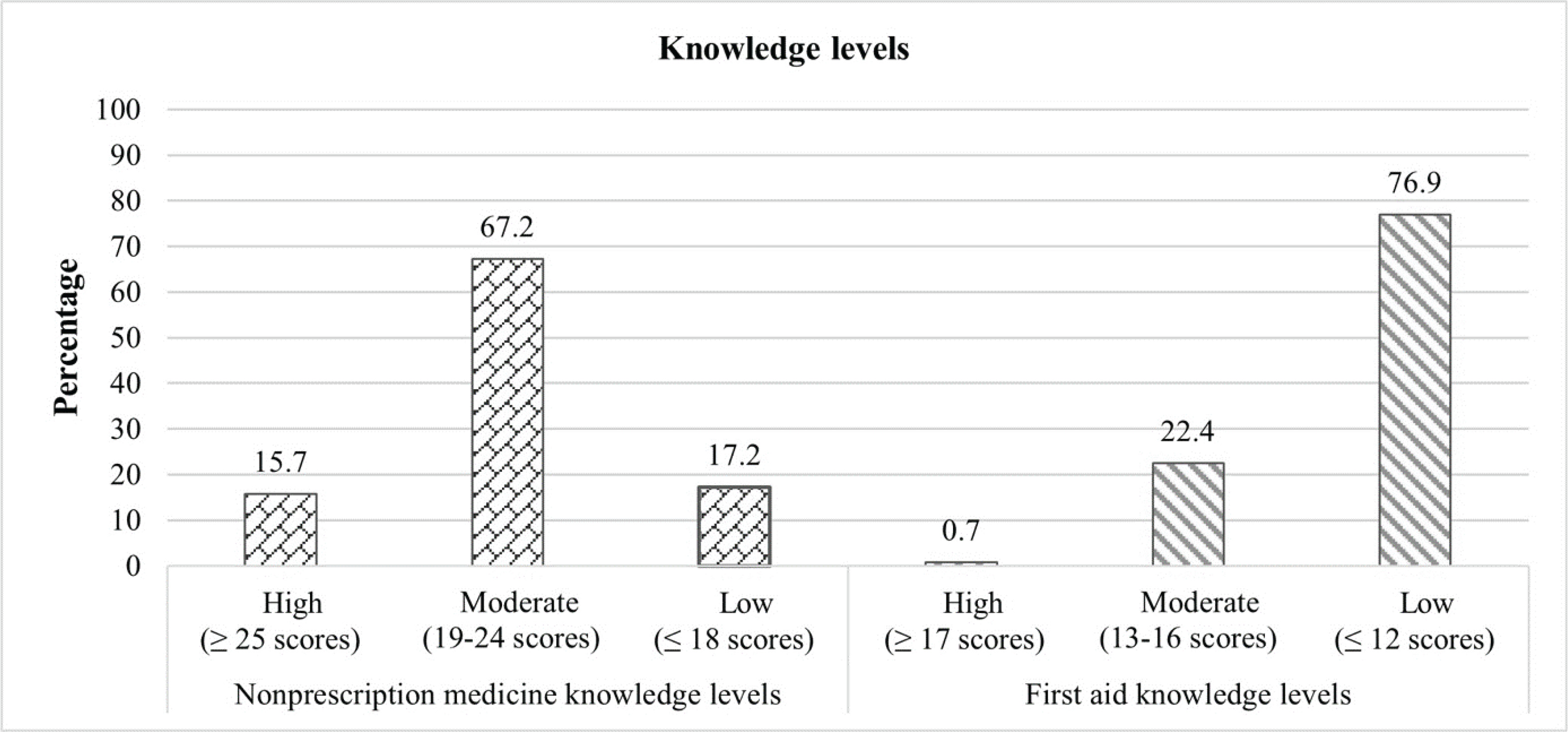
Among the participants, nearly two-thirds (67.2%) were categorized with moderate levels of nonprescription medicine knowledge, while only 15.7% demonstrated high proficiency. Additionally, more than three-fourths of the participants (76.9%) displayed limited proficiency in first-aid knowledge, with 0.7% demonstrating high proficiency (Figure 2).
Univariable and multivariable linear regression analyses were used to analyze variables associated with nonprescription medicine knowledge. In univariable linear regression analysis, age, years of experience in teaching, years of experience in school health services, previous nonprescription medicine training, and previous first-aid training were found to be significantly associated with knowledge (p<0.15) (Table 2). Concerning the multicollinearity between age and years of experience in teaching, only years of experience in teaching variables was included in the model based on insights from the literature review and high correlation. Consequently, four variables were entered into the multivariable linear regression. The results of the final multivariable linear regression model revealed that years of experience in school health services and previous nonprescription medicine training were significantly associated with the knowledge of primary school health teachers toward nonprescription medicine (p<0.05; R2=0.225) (Table 3). There was a significant relationship between years of experience and scores in nonprescription medicine knowledge: every additional year of experience in school health services could increase the knowledge score in nonprescription medicine by about 0.110 points (β=0.225, 95% CI: 0.023–0.198, p<0.013). Moreover, the model predicted that the score for nonprescription medicine knowledge was 1.806 points higher for the primary school health teachers who had previous nonprescription medicine training compared to those who did not have such previous training (β=0.270, 95% CI: 0.628–2.98, p=0.003).
Table 2
Factors associated with nonprescription medicine knowledge among school health teachers by univariable linear regression
| Variables | B | SE | β | p | 95 % CI |
|---|---|---|---|---|---|
| Gender | |||||
| Male ® | |||||
| Female | -0.05 | 0.97 | -0.004 | 0.96 | -1.98–1.88 |
| Age (years) | 0.07 | 0.02 | 0.24 | 0.005* | 0.02–0.12 |
| Education level | |||||
| Diploma ® | |||||
| Bachelor’s degree | -1.32 | 2.12 | -0.20 | 0.53 | -5.51–2.87 |
| Postgraduate | -0.80 | 2.15 | -0.12 | 0.71 | -5.05–3.46 |
| A degree related to health sciences | |||||
| No ® | |||||
| Yes | 1.35 | 1.73 | 0.07 | 0.43 | -2.06–4.77 |
| Years of experience in teaching | 0.07 | 0.02 | 0.26 | 0.002* | 0.03–0.12 |
| Years of experience in school health services | 0.17 | 0.04 | 0.35 | <0.001* | 0.09–0.25 |
| Previous nonprescription medicine training | |||||
| No ® | |||||
| Yes | 2.51 | 0.54 | 0.38 | <0.001* | 1.44–6.58 |
| Previous first-aid training | |||||
| No ® | |||||
| Yes | 1.60 | 0.50 | 0.27 | 0.002* | 0.60–2.59 |
| Number of teaching subjects | -0.01 | 0.03 | -0.03 | 0.76 | -0.06–0.05 |
| Number of teaching hours per week | 0.04 | 0.04 | 0.09 | 0.32 | -0.04–0.11 |
Table 3
Factors associated with nonprescription medicine knowledge among school health teachers by multivariable linear regression
| Variables | B | SE | β | p | 95% CI | VIF |
|---|---|---|---|---|---|---|
| Constant | 17.45 | 0.84 | <0.001* | 15.79–19.10 | ||
| Year of experience in teaching | 0.03 | 0.02 | 0.09 | 0.30 | -0.02–0.07 | 1.31 |
| Year of experience in school health services | 0.11 | 0.04 | 0.23 | 0.01* | 0.02–0.20 | 1.35 |
| Previous nonprescription medicine training | 1.32 | |||||
| No ® | ||||||
| Yes | 1.81 | 0.60 | 0.27 | 0.003* | 0.63–2.99 | |
| Previous first-aid training | 1.32 | |||||
| No ® | ||||||
| Yes | 0.49 | 0.53 | 0.08 | 0.36 | -0.57–1.54 |
For the outcome of the first-aid knowledge testing, four variables were considered. (Table 4). The results in the final model revealed that years of experience in school teaching, previous nonprescription medicine training, and previous first-aid training were significantly associated with first-aid knowledge (p<0.05; R2=0.435) (Table 5). There was a significant relationship between years of teaching and scores in the first-aid knowledge test (β=0.339, 95% CI: 0.002– 0.076, p=0.040). Moreover, each incremental point in the first-aid knowledge score was associated with an increase of approximately 3.830 points (β=0.700, 95% CI: 3.009–4.652, p<0.001). Interestingly, school health teachers with previous nonprescription medicine training exhibited lower scores in first-aid knowledge compared to those without such training (β= -0.177, 95% CI: -1.997 – -0.161 p=0.022).
Table 4
Factors associated with first-aid knowledge among school health teachers by univariable linear regression
| Variables | B | SE | β | p | 95% CI |
|---|---|---|---|---|---|
| Gender | |||||
| Male ® | |||||
| Female | 0.09 | 0.89 | 0.01 | 0.92 | -1.67–1.85 |
| Age (years) | 0.04 | 0.02 | 0.14 | 0.11* | -0.01–0.08 |
| Education level | |||||
| Diploma ® | |||||
| Bachelor’s degree | 0.95 | 1.94 | 0.16 | 0.62 | -2.88–4.78 |
| Postgraduate | 1.23 | 1.97 | 0.21 | 0.53 | -2.66–5.12 |
| A degree related to health sciences | |||||
| No ® | |||||
| Yes | 0.47 | 1.58 | 0.03 | 0.75 | -2.63–3.62 |
| Years of experience in teaching | 0.04 | 0.02 | 0.16 | 0.06* | -0.002–0.08 |
| Years of experience in school health services | 0.09 | 0.04 | 0.20 | 0.02* | 0.02–0.17 |
| Previous nonprescription medicine training | |||||
| No ® | |||||
| Yes | 1.04 | 0.52 | 0.17 | 0.05* | 0.01–2.08 |
| Previous first-aid training | |||||
| No ® | |||||
| Yes | 3.45 | 0.37 | 0.63 | <0.001* | 2.72–4.18 |
| Number of teaching subjects | 0.01 | 0.02 | 0.04 | 0.63 | -0.04–0.06 |
| Number of teaching hours per week | -0.01 | 0.03 | -0.03 | 0.78 | -0.08–0.06 |
Table 5
Factors associated with first-aid knowledge among school health teachers by multivariable linear regression
| Variables | B | SE | β | p | 95% CI | VIF |
|---|---|---|---|---|---|---|
| Constant | 5.91 | 0.65 | <0.001* | 4.62–7.19 | ||
| Years of experience in teaching | 0.04 | 0.02 | 0.16 | 0.04* | 0.002–0.08 | 1.31 |
| Years of experience in school health services | -0.004 | 0.03 | -0.01 | 0.90 | -0.07–0.06 | 1.35 |
| Previous nonprescription medicine training | ||||||
| No ® | ||||||
| Yes | -1.08 | 0.46 | -0.18 | 0.02* | -1.10 – -0.16 | 1.32 |
| Previous first-aid training | ||||||
| No ® | ||||||
| Yes | 3.83 | 0.42 | 0.70 | <0.001* | 3.01–4.65 | 1.32 |
DISCUSSION
The present study represents the first attempt to assess the knowledge of nonprescription medicine and first aid among primary school health teachers in Northern Thailand. Additionally, this study investigates the factors associated with school health teachers. The findings presented are of great significance and provide valuable insights.
This study revealed a notable deficiency in the understanding of primary school health teachers regarding nonprescription medicine. Only 15.7% of the participants exhibited a high level of knowledge, whereas 17.2% demonstrated a low level of knowledge. Despite efforts by various regulatory agencies to enforce guidelines aimed at ensuring the safe use of nonprescription medications in the absence of medical supervision, concerns persist regarding the potential for misuse among individuals who assume the role of caregivers for school children during school hours. This misuse specifically refers to the improper administration of medications for legitimate medical purposes, encompassing errors in dosage, dosage form, frequency, and duration17.
The study findings indicate a statistically significant correlation between primary school health teachers’ levels of prior training in nonprescription medicine and their levels of knowledge. These results underscore the importance of providing training to primary school health teachers in nonprescription medicine procedures. It is crucial for these teachers to continually update their knowledge and skills in accordance with the current guidelines for nonprescription medicine. By doing so, they can effectively fulfill their roles and responsibilities in promoting the safe and appropriate use of nonprescription medications among school children16,18. Moreover, the study findings demonstrate a significant association between the experience of primary school health teachers in school health services and their levels of knowledge of prescription medications. The results suggest that teachers who had previous experience in administering medications for chronic illnesses to children in their own schools were more inclined to adopt the best practices related to nonprescription medicine. This highlights the potential influence of practical experience in fostering better understanding and application of nonprescription medication-related knowledge among teachers in the school health setting.
The present investigation revealed that approximately three-fourths of the participants had a low level of first-aid knowledge. This finding aligns with a study conducted in Hawassa City, Southern Ethiopia, which indicated that a majority of primary school health teachers lacked knowledge about first-aid measures29. However, the prevalence of low knowledge in this study was higher than that reported in a study conducted in Kashan, Iran, where no participant had a high level of first-aid knowledge, but 63.3% and 36.7% exhibited moderate or weak first-aid knowledge, respectively23. Similarly, a study conducted in Kerbala City, Iraq, indicated that most primary school teachers had a low level of first-aid knowledge (50.0%)30. Studies conducted in Addis Ababa and Debre Tabor City, Ethiopia, also reported that more than half of the school health teachers lacked knowledge of first aid4,19. These findings are consistent with a previous systematic review that highlighted inadequate first-aid knowledge among school health teachers21. These findings imply that inappropriate knowledge of first aid among school health teachers may decrease the chances of children receiving appropriate and timely first aid, which could potentially increase the risk of complications after any incident in the school environment. Therefore, policymakers have a responsibility to plan and implement first-aid teaching programs for all school teachers or, at the very least, for selected teachers from each school23.
In our study, the multivariable linear regression analysis revealed a positive association between teaching experience and knowledge of first aid. This observation aligns with the results obtained in a previous study conducted in Athens, Greece31; Port Said city, Egypt32; Gondar city, Northwest Ethiopia20; Al-Najaf Al-Ashraf city, Iraq24; Riyadh, Saudi Arabia33; and Malatya, Turkey34, which demonstrated that longer teaching experience was significantly associated with higher levels of first-aid knowledge among participants. Nevertheless, several studies conducted in different regions, including Iraq24, Iran23, Southern Ethiopia29, and Nigeria35, have reported contrasting findings. These studies found no significant association between teaching experience and first-aid knowledge among school health teachers. These divergent outcomes suggest that the relationship between teaching experience and first-aid knowledge may vary across different contexts and settings. The disparities observed in the findings of these studies can be attributed to several factors, including variations in the characteristics of the study samples, settings, and the availability and effectiveness of teacher preparation and in-service programs across different countries. These differences emphasize the significance of contextual factors and educational interventions in shaping the relationship between teaching experience and first-aid knowledge among school health teachers. Therefore, it is crucial to acknowledge and consider these contextual variations when interpreting the results of these studies.
In this study, it was found that more than half of the participants had previous first-aid training. This finding is consistent with studies conducted in Al-Najaf Al-Ashraf City, Iraq (60.9%)24 and Uttarakhand, India (72.0%)25. However, the prevalence of previous first-aid training in this study was higher compared to studies conducted in Dura city, Palestine (42.0%)22; Kashmar, Iran (40.3%)23; Debre Tabor city, Northwest Ethiopia (35.2%)19; Addis Ababa, Ethiopia (32.0%)4; Karnataka, India (30.2%)36; Gondar city, Northwest Ethiopia (28.4%)20; Hawassa city, Southern Ethiopia (25.4%)29; and Kerbala city, Iraq (10.0%)30. These variations in the prevalence of previous first-aid training among participants across different studies and locations may be attributed to differences in the availability and accessibility of first-aid training programs, cultural and educational factors, and the emphasis placed on first-aid training within specific regions or institutions. It is important to consider these differences when interpreting the findings and designing interventions to improve first-aid knowledge and training among school health teachers.
Our study findings indicate a positive association between previous training in first aid and knowledge of first aid among school health teachers. This result is in line with a study conducted in Addis Ababa, Ethiopia, which reported that school health teachers who had received prior first-aid training demonstrated levels of knowledge that were approximately three times higher compared to those without such training. These consistent findings suggest that formal training in first aid plays a crucial role in enhancing the knowledge of school health teachers in this domain4. Several previous studies have provided support for this association, demonstrating a significant correlation between prior first-aid training and knowledge19,29,31,37. These findings suggest that training plays a vital role in increasing the knowledge of school health teachers in first aid. Moreover, individuals who have received training in first aid are likely to be more confident and motivated to provide assistance during incidents that occur in school settings. On the other hand, individuals who have not received specific first-aid training may be more hesitant to offer help during critical incidents23. However, it is important to acknowledge that certain studies conducted in specific regions such as Gondar City, Northwest Ethiopia20, and Malatya, Turkey34, did not demonstrate a significant association between previous first-aid training and knowledge. These differences in findings may be attributed to variations in the method and depth of training provided to school health teachers. Overall, the evidence suggests that providing comprehensive and effective first-aid training programs to school health teachers is essential in improving their knowledge and ensuring their readiness to respond to emergencies in school environments. Based on the study’s findings, several organizational policies could be developed to elevate the levels of nonprescription medicine and first-aid knowledge among school health teachers. Specifically, the education sector should consider implementing policies that endorse the necessity for school health teachers to undergo training, including the certification of such training. Additionally, the public health sector could contribute by providing a training curriculum and regularly updated information resources regarding nonprescription medicine and first-aid knowledge for school health teachers.
Limitations
This study is not without limitations. Firstly, because of the cross-sectional design, no causal inferences can be drawn from the observed associations as the study captures information at specific time points. Secondly, relying on self-reported data introduces the possibility of biases such as recall bias and social desirability bias. Thirdly, preventing teachers from refreshing their knowledge before completing the questionnaire poses a challenge, as they are aware of being surveyed. Nevertheless, the researcher emphasized to the teachers the importance of grasping the true situation. They were assured that the scores would be presented collectively, without impacting their individual performance. Lastly, the study was conducted within a single province, limiting the generalizability of the findings to a broader population. To address these limitations, future research should involve large-scale, multicenter studies to examine the nonprescription medicine and first-aid knowledge of school health teachers on a nationwide level. Moreover, the lack of sufficient numbers of similar studies at the national level hinders the scope for meaningful comparisons. Further investigation is necessary to overcome these limitations and provide a more comprehensive understanding of school health teachers’ first-aid knowledge.
CONCLUSIONS
The results of this study emphasize the importance of experience and specialized training in improving the knowledge and skills of primary school health teachers in these areas. Enhancing their expertise can contribute to significantly better health outcomes for students and provisions of effective care in school settings. We recommend implementing policies in the education sector mandating training and certification for school health teachers, while the public health sector could offer a training curriculum and updated resources on nonprescription medicine and first-aid knowledge.