

INTRODUCTION
Cigarette smoking has been a significant risk factor for cancer and chronic disease development for over half a century1. Since 2007, e-cigarettes and vaping have emerged as additional public health burdens alongside combustible smoking, enticing both cigarette smokers and non-cigarette youth and young adult smokers with their appealing marketing and flavors2. Youth and young adults are predominant users of e-cigarettes as 5.9% of middle and high school students used e-cigarettes in 2024 and 10.3% of young adults aged 18–20 years and 15.5% of young adults aged 21–24 years in 20233,4. Although vaping has been promoted as a healthier alternative to combustible tobacco, its long-term health effects remain insufficiently understood5. Cigarette smoking cessation programs have demonstrated effectiveness in supporting individuals to reduce or quit smoking through various interventions, including individual counseling, group therapy, behavioral treatments, and pharmacotherapies6.
Despite the development of smoking cessation programs, many barriers limit uptake and adherence. Barriers include insufficient awareness of available services, transportation issues, scheduling conflicts, financial constraints, and inadequate insurance coverage7,8. Clinical and psychological barriers, including withdrawal symptoms, relapse risk, undertreatment, lack of motivation, and cessation program stigma, can further discourage smokers from seeking support9,10. For marginalized communities, these barriers are compounded by members smoking as a coping mechanism for stress and adversity, facing peer pressure from the normalization of smoking within their social spheres, and receiving inadequate support from their healthcare providers11-16. These barriers disproportionately affect marginalized populations, exacerbating health disparities in smoking cessation outcomes among racial and ethnic minorities, LGBTQ+ communities, individuals with lower socioeconomic status and poor mental status, and at-risk youth17. Addressing these disparities requires engaging marginalized communities as active partners in participatory research, where they can co-develop and co-lead culturally tailored smoking cessation interventions that reflect their lived experiences and address their specific needs18. Furthermore, participatory research is more effective than traditional tobacco control and cessation programs in raising awareness and building trust within community spaces due to cultural competency19.
Photovoice exemplifies this participatory research framework through empowering individuals as co-researchers who use photography and written storytelling20,21. Photovoice invokes creativity and allows participants to showcase their individual understandings of the social pressures, environmental factors, and obstacles that shape their experiences with smoking and cessation regulations22. Through capturing images of tobacco marketing, policy enforcement, and cessation resources in their communities, participants illuminate the stigma, stress, and systemic barriers that hinder program adherence with greater emphasis than traditional research methods provide.
Moreover, photovoice fosters collaboration between community members and researchers by promoting critical reflection on shared insights and supporting advocacy for improved smoking cessation policies23. Photovoice methodology has been in practice since at least 1992, and since then has been extensively refined and implemented within community-based participatory research (CBPR) initiatives to support health promotion across diverse health issues, including diabetes, HIV prevention, cancer, and mental health. Within CBPR research, photovoice has helped rebuild trust and accountability between community members and policymakers by highlighting community experiences, concerns, and shifting priorities to be beyond the scope of behavioral health questionnaires24. Integrating photovoice into mixed-methods research with marginalized communities can create space for community solidarity and enhanced cultural competency25. Thus, the application of photovoice in tobacco control and smoking cessation research can promote more suitable and equitable interventions tailored to marginalized communities.
Although photovoice has been applied in research involving other areas of disease prevention and modifiable behavioral factors, its use and impact within smoking cessation research have been more limited21-25. The goal of this scoping review is to make an inventory and analyze photovoice-related interventions conducted with individuals who currently smoke or vape, have recently quit smoking or vaping, or are at-risk for smoking from environmental influences to answer the following questions: 1) ‘What research aims are being addressed using photovoice methods in diverse populations regarding smoking behavior and cessation programs?’; 2) ‘What demographic variations exist in the included studies?’; 3) ‘What are the key themes that arose during photovoice research?’; and 4) ‘What impact did photovoice have on behavioral health choices and policy regarding smoking behaviors, tobacco control, and smoking cessation programs?’.
METHODS
This review followed the methodological framework for scoping reviews outlined by Arksey and O’Malley26,27. We conducted the literature review through the following steps: 1) develop a research question; 2) create a comprehensive search strategy to identify relevant studies; 3) define inclusion and exclusion criteria for relevant studies; 4) chart and extract the data; and 5) collate, summarize, and report the results through thematic analysis. Keywords and medical subject headings (MeSH) terms related to photovoice and smoking prevention and cessation were identified. Independently, we facilitated a comprehensive search across the following six databases: PubMed, MEDLINE through Ovid, CINAHL, EMBASE, PsycINFO, and Web of Science. An example of the Boolean operators and search terms used in the PubMed database is shown in Supplementary file Table 1.
Table 1
Summary of details of included studies in the scoping review, 26 June 2025
| Author Year | Location | Database and last search date | Sample size | Age of participants | Smoking status of participants | Participant characteristics | Aims | Research question(s) | Photovoice training and instructions | Study design | Main communication goals | Key themes and main findings |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Chopel et al.29 2019 | Oakland California USA | CINAHL 17 June 2025 | 3 | 14-24 years old | Not specified | Youth and young adult community members who live, work, or study in the racially/ethnically and socioeconomically diverse city of Oakland | Qualitative | How are e-cigarettes marketed and promoted to youth in Oakland? How are these products perceived by youth in Oakland? | The research team from California Adolescent Health Collaborative (CAHC) and University of California San Francisco (UCSF) trained youth coresearchers in photovoice basics, e-cigarette marketing, and research ethics. They used personal cell phones to photograph e-cigarette marketing risks and protective factors daily for 21 days, creating narratives using the SHOWeD methods. | Qualitative: photovoice activity, geo-narrative mapping, steering committee analysis, and SHOWeD method | Health advocacy, youth empowerment, policy change, awareness raising | Tobacco and e-cigarette companies enticed youth with their versatile flavors and colorful catchy phrases. The prominence of products in stores and eye-level placement were strategic marketing tactics. Participants engaged in community advocacy, presented their photos from the META-Oak Project at conferences, and contributed to a ban on flavored tobacco sales. |
| Haines-Saah et al.30 2013 | Vancouver Canada | PubMed 26 June 2025 | 12 | 19-26 years old | Recently quit smokers attempting cessation | The majority of participants (eleven) were full-time post-secondary students with no specific identification as coming from marginalized communities | Exploratory | How do localized discourses on ‘healthy living’ and socio- spatial contexts in Vancouver influence participants’ experiences as smokers and their attempts at cessation? | Young adults received a disposable camera from the research staff and were instructed to imagine themselves contributing to an exhibition titled ‘Smoking & Quitting—My Views.’ They captured aspects of their tobacco experiences. Participants wrote captions for 3-5 images and then discussed them in a photo interview. | Qualitative: photovoice activity, interviews, and focus groups | Awareness raising, empowerment, education | Vancouver’s emphasis on leading a healthy lifestyle pressures people to assimilate to the dominant culture of cessation, yet the process can feel exclusionary and a major lifestyle change. Outdoor spaces were viewed as places for smoking freely, but also avenues for strengthening physical activity. |
| Hanby et al.31 2023 | Online recruitment nationwide in the USA | CINAHL 17 June 2025 | 47 | Mean age is 26 years | Current smokers: split between daily and occasional | The majority of participants identified as non-heterosexual, transgender, and gender- diverse (TGD), and/or employed | Exploratory | What are the experiences of TGD individuals regarding the risk and protective factors influencing their smoking habits, using a photovoice methodology? What is the feasibility of enrolling and engaging TGD individuals in a digital photovoice study to gather this information? | Participants were instructed by the research team to use Facebook and Instagram closed groups to post pictures of smoking risks and protective factors they encountered in their daily lives over a 21-day period. They were also encouraged to comment on and react to other participants’ posts. A focus group was followed to discuss the images. | Mixed-Methods: photovoice activity, focus groups, feasibility scale (quantitative), counts data of digital media engagement (quantitative) | Awareness raising, empowerment | Using Facebook and Instagram for their smoking cessation photovoice project helped researchers recruit a wider network of TGD adults. It also built a strong community within focus groups and allowed participants to feel comfortable sharing insights on their smoking habits through daily reflection prompts on social media. Participants received better engagement on Instagram (average of 27 comments/person) as compared to Facebook (average of 2.5 comments/person) for 3 weeks. |
| Jardine et al.32 2012 | K’álemì Dene School and Kaw Tay Whee School in Ndilo and Dettah Northwest Territories Canada | PubMed 12 June 2025 | 48 | 7-19 years old | Smokers, nonsmokers, and former smokers | Indigenous schoolaged children | Exploratory and Qualitative | What do youth know and understand about tobacco use? How do youth view tobacco use in their community? What influences youth’s decisions to start smoking or not to start smoking? | High school participants were given disposable cameras by the collaborative research team to take pictures of tobacco use in their community. They were also briefed on ethics, interview question development, and digital recording. For photovoice, they took pictures related to smoking (positive/negative, community views) and avoided people without permission or smoking. | Qualitative: photovoice activity and interviews | Awareness raising, empowerment | Participants created a book entitled Youth Voices on Tobacco, which was distributed at the schools. Youth researchers paired negative pictures with positive depictions to better persuade others to conform to the desired healthy behavioral changes of quitting smoking. Youth researchers had the opportunity to improve their research and leadership skills and raise awareness on smoking habits for the rest of the community members. |
| Lee et al.33 2019 | San Francisco Bay California USA | CINAHL 17 June 2025 | 5 | 15-24 years old | Not specified | A multi-ethnic subgroup of youths from the Southeast Asian Young Leaders (SEAYL) program | Intervention and Exploratory | How does tobacco use impact the community of youths in the SEAYL program? What are the processes through which youth participants developed critical consciousness and assessed their experiences within their community’s tobacco environment? | Academic and community partners trained youth over six weeks on photovoice methodology, basic photography, techniques, and the SHOWeD framework. They photographed tobacco advertising in areas near their schools. Participants also photographed locations where they had witnessed frequent tobacco use before, during, and after school hours. Then participants discussed their photos using the SHOWeD method and wrote captions. | Standalone: photovoice, focus groups, SHOWeD method | Awareness raising | Youth and young adults developed more critical awareness of their surroundings and strengthened their connections with different community members with regard to their tobacco environment. The main themes that emerged from the photos captured were: negative environments, lack of no-smoking enforcement at school, lack of signage, negative perceptions and attitudes, and positive environments. Photovoice facilitated conversation surrounding socioeconomic hardships hinder self-efficacy in combating tobacco use. |
| Mermer et al.34 2024 | Vocational and Technical Anatolian High School Turkey | PubMed 26 June 2025 | 395 | Median age is 15 years | Smokers and non-smokers | Majority of participants were school-aged males from a disadvantaged district | Intervention | Does peer education improve knowledge, reduce smoking frequency, and enhance health literacy among high school students from disadvantaged school districts? | Peer educators were trained by photography experts in photovoice methods and led peer discussions on ethics and methodology. Students then took photos for four months, discussed them to create stories, and exhibited selected photos. | Mixed-Methods: smoking frequency (quantitative), levels of health literacy (quantitative), tobacco use, photovoice activity, and narrative data | Health education, behavior change with reducing smoking, empowerment for youth to become advocates and health educators, awareness raising | Youth were primarily seeking to identify how social, cultural, and environmental factors and sale conditions affected their tobacco use and if they saw a relationship between tobacco and cancer through photovoice. Smoking rates (33.0% to23.0%) and indoor cigarette smoking rates (54.5% to 45.2%) were reduced with the implementation of the peer educator and photovoice education program for the disadvantaged students in Turkey. Their health literacy scores significantly improved post intervention (p<0.05) as well. |
| Mitchell et al.35 2021 | Three rural counties in a southern mid-Atlantic state USA | PubMed 12 June 2025 | 13 | 25-57 years old | Current and former smokers | Women from low- income, rural backgrounds, with majority identifying as African American | Exploratory | What are the social and cultural factors that give meaning to smoking in rural low-income women? What is the relationship between these social and cultural factors, social support, social networks, and social identity in their decisions to smoke or attempt smoking cessation? | The primary investigator provided cameras/phones to participants. Instructions included taking photos daily for 2-6 weeks and providing meaningful titles. Consent for others in photos was mandatory and explained. There was also a second visit by the primary investigator to the participant’s home to complete a follow-up semistructured interview. The participantproduced photos were used during the second interview as a means of eliciting deeper discussion and gaining insight into what it means to smoke and be a smoker. | Qualitative: artifact collection, photovoice activity, fieldnotes, memos, narrative data, and thematic analysis | Empowerment | Smoking was used as a coping mechanism for stress relief, daily struggles, and isolation, and was often normalized for families that also smoked. This normalization interfered with cessation plans due to the comfort and relaxation smoking provided them. Smoking was considered unacceptable in public spaces, and the topic was not discussed in front of family members, friends, or the church. Others felt pressure to quit to ‘look good’ and were motivated by being good mothers and preventing a smoking habit for their children. Throughout the pictures and narratives in photovoice were visions, expectations, and plans for a better life that would enable these women to quit smoking. |
| Oliffe et al.36 2010 | Vancouver British Columbia Canada | CINAHL 17 June 2025 | 20 | 22-41 years old | Smokers and recently quit smokers | All were fathers who smoked during their partners’ pregnancy and almost half identified as Asian or of Middle Eastern descent. | Exploratory and Qualitative | What are the locations and contexts that facilitate and restrict participants’ smoking behaviors within the context of fatherhood? | Researchers gave fathers disposable cameras after an initial interview, instructing them to photograph places they smoked for an exhibition titled ‘Smoking Through the Eyes of Fathers.’ A second interview involved discussing each photo with open-ended questions. | Qualitative: photovoice activity, interviews, transcripts, and field notes | Education, awareness-raising, and advocacy | Workplace smoking was normalized as a therapy for bosses to control their aggression and as a ritualistic group experience. Smoking also became more commonly done at work for fathers with pregnant partners to reduce stress, spend free time, and reward their achievements. Moreover, fathers avoided smoking in the home because of the presence of a baby, but they used the balconies, porches, adjoining alleys, and parking lots instead. Their smoking practices were intertwined with their masculinities. |
| Petteway et al.37 2019 | Southwest Baltimore Maryland USA | PubMed 4 June 2025 | 14 | 5th to 8th graders | Not specified | Middle school students from a racially diverse, high-tobacco-burden, low-income, urban community | Exploratory and Qualitative | How do youth from Southwest Baltimore perceive tobacco-related issues and what shapes their interactions with their local tobacco environment? How can youth serve as agents of change for intergenerational tobacco cessation programs? | Facilitators recruited 14 youth and provided two training sessions on participatory research, digital camera use, and ethics. Youth took independent photos on ‘tobacco environment and community health,’ then used both SHOWeD and PHOTO techniques for narratives and discussion. | Qualitative: photovoice activity, group facilitated discussions, thematic analysis, SHOWeD method | Awareness raising, youth empowerment, community advocacy, fostering intergenerational dialogue and understanding | The CEASE CBPR project facilitated critical reflection and dialogue surrounding smoking prevention and cessation among youth and young adult coresearchers. Photovoice revealed the following prominent themes: harmful nicotine addictions, strategic marketing tactics through enticing others to purchase cigarettes, food insecurity in the community from overconsumption of tobacco products, and health promotion materials to reduce smoking in communities. This was the first youth-led tobacco-resistant project in Southwest Baltimore at the time of the project, and it was presented at City Hall. This project led to the formation of the Youth Tobacco Advisory Council in 2014 and has advocated for numerous tobacco control policies. |
| Seitz et al.38 2012 | A large, public 4-year university in the Southeast region of the United States | MEDLINE 5 June 2025 | 49 | Mean age of 18-22 years | Not specified | Undergraduate students enrolled in a public health education course with no specific identification as coming from marginalized communities | Qualitative | How can photovoice empower college students to advocate for change in smoking policy on campus? | Undergraduates enrolled in a Public Health Education course were provided six 1-hour training sessions covering the overview of tobacco use and health policy, ACHA recommendations, and an overview of photovoice. Participants were provided with disposable and digital cameras. They were also trained in the SHOWeD method for discussion and analysis. | Qualitative: photovoice activity, thematic analysis, and SHOWeD method | Awareness raising, advocacy, education | Photovoice empowered university students to advocate for changes in smoking policy on their campus after identifying aesthetic concerns, policy violations, secondhand smoke exposure, and smokeless tobacco littering. Ashtrays in violation of campus policies were removed shortly after the photovoice exhibitions and others quit smoking upon project completion. |
| Tanjasiri et al.39 2013 | Long Beach and Pasadena California USA | PubMed 5 June 2025 | 32 | 15-25 years old | Smokers and non-smokers | Asian American and Pacific Islander (AAPI) youth leaders engaged in community-based organizations | Qualitative | How can photovoice and GIS mapping be used to help AAPI youth understand and uncover environmental disparities from tobacco use? | CBO organizations involved 32 CBPR-trained youth leaders to photograph community locations influencing tobacco use. They later analyzed the photos using the SHOWeD mnemonic. Participants developed written analyses of each picture they captured on their cameras. | Mixed-Method: Geographic Information System (GIS) mapping, photovoice activity, individual youth surveys, and SHOWeD method | Awareness raising, empowerment, advocacy, and community capacity building | AAPI youth and young adults identified four environmental factors for smoking: youth-targeted cigarette advertisements, abundance of smoke shops showcasing cigarette advertisements, poor physical appearance of their community, and anger at tobacco companies that profited from their community. Photovoice integrated within CBPR facilitated advocacy through youth leadership programs that pushed for the tobacco retailer permit ordinances. |
| Woodgateet al.40 2015 | Western Canada | PubMed 12 June 2025 | 75 | 11-19 years old | Smokers, former smokers, and non-smokers | Canadian youth from urban centers and rural areas with no specific identification as coming from marginalized communities | Qualitative | How do Canadian youth perceive smoking among their peers and how does it affect their relationships with their peers? | Research assistants provided disposable cameras to youth who photographed people, objects, places, or events related to cancer and prevention for 3-5 weeks. Discussions followed the SHOWeD method. | Standalone qualitative: interviews, photovoice activity, focus groups, and SHOWeD method | Awareness raising, youth empowerment, health promotion, and peer pressure resistance | Photovoice helped youth understand the influence of smoking on relationships. Peers took up smoking because they felt they emulated the energy of ‘coolness’. Friends had to navigate how to balance being influenced to smoke or being the influencer who quit or put pressure on smoking. Additionally, peers could better decipher which of their friends smoked and why they chose to. Finally, participants reflected that setting boundaries and rules with their peers who smoke can help protect and empower themselves to protect and empower themselves to resist temptations or influences to smoke. |
Since search parameters varied by database, the format of operators and key terms was modified accordingly for each database to optimize the retrieval of relevant studies. Results were limited to studies published prior to 1 June 2025, and no additional filters or restrictions were applied. References of relevant articles were reviewed, and Google Scholar was used to identify other eligible studies.
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) process was conducted (SK and DR) in Covidence for screening articles for inclusion in the review28. Prior to the initial screening for titles and abstracts, all references were downloaded into Zotero for detection and removal of duplicates. Article titles and abstracts were first extracted and reviewed independently by both researchers to determine which ones met the inclusion criteria by key terms. Full text was subsequently analyzed, and the inclusion criteria were applied throughout; any disagreement was discussed following independent review and resolved together afterwards.
As described in a PICO table (Supplementary file Table 2), studies were included in the review if they met the following criteria: 1) focused on nicotine-based smoking (tobacco smoking, e-cigarettes, vaping, or hookah use) as the primary outcome; 2) integrated photovoice as a method for bolstering health education, health literacy, and health advocacy whether it be as a standalone method or in conjunction with other mixed-method approaches; 3) published in English as peer-reviewed studies; and 4) no parameterization on population demographics. Studies were ineligible for inclusion if they; were published in a foreign language; were review articles, editorials, book chapters, dissertations, and conference abstracts; or not published in a peer-reviewed journal.
Key components of each study were extracted from the text and organized in spreadsheets, including first author, year of publication, location of study, sample size, age of participants, type of community group, research aims, research question, photovoice training and instructions, data collection methods, main communication goals, and main findings of each individual study. The data extraction was conducted by both reviewers and any discrepancies were addressed among the research team.
RESULTS
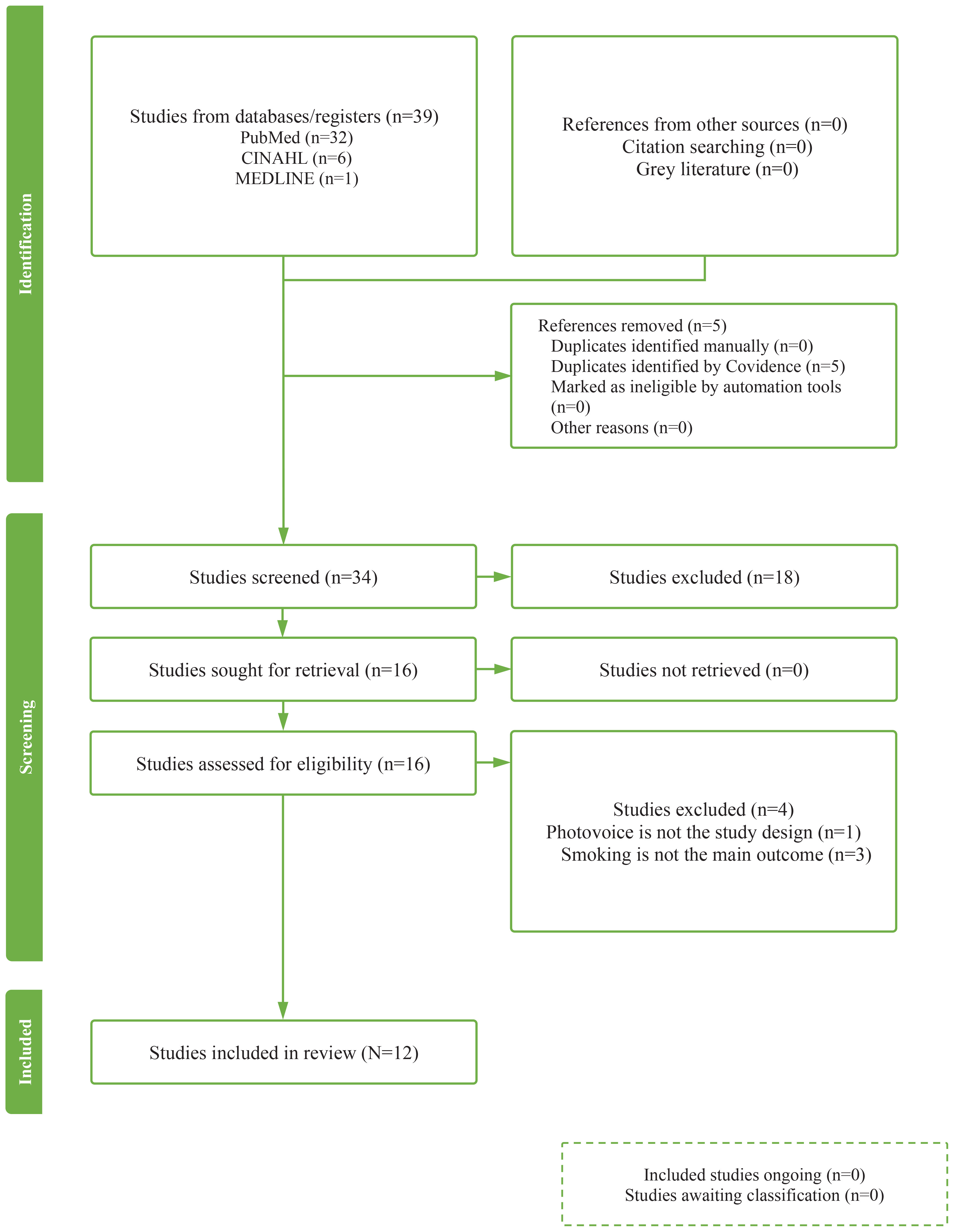
Figure 1 demonstrates the process of selecting articles guided by the PRISMA framework. The search identified 39 articles from the selected databases. After the removal of duplicates, 34 studies were screened in the title and abstract stage. Of these, 16 full-text articles were assessed for eligibility by all inclusion parameters. Four articles were removed in the full-text review: three articles did not have smoking as the primary outcome and one article implemented an inappropriate study design. In the end, 12 studies were reported and analyzed in the scoping review, as delineated in Figure 129-40.
Figure 1
The PRISMA diagram of our scoping review on peer-reviewd studies focused on the incorporation of photovoice in smoking prevention and cessation published before June 1, 2025
Characteristics of included studies
All identified studies from our extraction stage were published between 2010 and 2024 and conducted in the United States (n=7), Canada (n=4), and Turkey (n=1). Participant ages ranged from 7 to 57 years with most studies concentrating on youth and young adult populations (ages 7–26 years). Sample size varied considerably from 3 to 395 participants with most enrolling less than 50 people30-32,35-39 Half of the studies recruited a mix of smokers, non-smokers, and recent quitters32,34-36,39-40, while one explicitly targeted recent quitters attempting cessation programs30 and another focused solely on smokers with daily or occasional tobacco consumption31. Four studies did not report participants’ smoking status29,33,37,38.
Nine studies predominantly recruited individuals from marginalized communities, including socioeconomically disadvantaged populations34-35,37, racial and ethnic minorities32-33,36,39, LGBTQ+ members31, and at-risk adolescents29,33. The remaining studies either did not recruit based on marginalized status or included cohorts that were not predominantly composed of marginalized individuals30,38,40.
Recruitment methodology also varied across the articles. Eight studies recruited participants directly from high schools, universities, and post-secondary schools30,32-34,37-40 and the other four studies used community organizations, health facilities, and digital campaigns to primarily enroll marginalized adults from low-income backgrounds, transgender and gender-diverse communities, and racial or ethnic minorities29,31,35-36. Comprehensive study design and participant characteristics are presented in Table 1.
Community engagement and partnerships
Five studies were structured as full CBPR initiatives with formal partnerships between researchers, community-based organizations (CBOs), and nonprofit organizations29,32,33,37,39. These partnerships utilized steering committees with representatives from public health agencies, local advocacy organizations, and community-based partners to guide the project design, recruitment, training, discussion, and dissemination activities and enabled shared decision-making between researchers, participants, and community stakeholders throughout the entire photovoice project. Additionally, participants served as co-researchers who deepened the collective understanding of tobacco control issues, local policies, and lived experiences surrounding smoking behaviors and cessation stigma. Only full CBPR studies reported sustained participant empowerment through continued advocacy with local and state advisory committees29,32 and community awareness campaigns presented to school administrators to address larger issues of tobacco use following project completion33,37,39.
Three studies partially implemented CBPR principles by centering participants as co-researchers and demonstrated enhanced insight into personal smoking behaviors and community tobacco control needs34-35,38. While these partial CBPR studies showcased immediate impact with increased health literacy on smoking consequences and personal empowerment34,35 and removal of ashtrays in violation of campus policies38, the extent, scale, and maintenance of this advocacy was limited in comparison to full CBPR studies. The remaining four studies that did not employ partial or full CBPR frameworks emphasized the benefits of photovoice for facilitating reflection on smoking experiences and self-empowerment but did not report comparable advocacy and community empowerment outcomes30-31,36,40.
Photovoice methodology and analysis
All articles provided training on photovoice usage, ethical photography guidelines, and subject consent. The devices used in photography varied greatly, as two studies used cell phones29,35, while five studies used disposable cameras30,32,36,38,40. The other studies used digital cameras35,37,38, did not specify the mechanism31,33-34, or did not specify the type of camera used39.
Our review also noted that the majority29,32,36-40 of the articles took a qualitative approach examining photovoice and smoking, with two also containing an exploratory approach32,36. Three of the remaining articles solely focused on exploratory analysis30,31,35, one article was exploratory and intervention-based33, and another article was solely intervention-based34.
Due to differences in study designs and photovoice activities, a variety of approaches were used to analyze participants’ narratives and photographs. For instance, some researchers used thematic analysis29,35 or a combination of both thematic and content analysis33. Photovoice often uses questions to describe the photographs and facilitate discussions. The following questions are asked: ‘What do you SEE here?’, ‘What is really HAPPENING here?’, ‘How does this relate to OUR lives?’, ‘WHY does this problem or situation exist?’, ‘How could this image EDUCATE others?’ and ‘What can we DO about it?’ These questions make up the SHOWeD mnemonic to describe photographs41. Six of the studies used this method to guide member reflections29,31,37-40. If the SHOWeD technique, thematic analysis, or content analysis were not explicitly stated, then the studies would conduct a similar analysis to the traditional methods30-32,34-36. Of the total amount, three had group discussions surrounding their findings with photovoice, which achieves the secondary goal of the activity20,21. Participants often met routinely to share what photovoice meant to them29,33,37. More information on the data collection methods and photovoice communication goals can be found in Table 1.
Key themes identified
All 12 studies showcased how photovoice elevated participants’ exploration of the social and environmental factors that influence smoking behaviors. Marketing emerged as a dominant pressure for youth and marginalized communities, as evidenced by participants’ photos and narratives documenting youth-targeted advertisements, colorful packaging, and strategic placement of tobacco and e-cigarette products in retail stores and throughout digital and physical community spaces29,31-35,37. Participants also emphasized how the flavored tobacco products and the brightly colored packaging also increased smoking temptations among youth and young adults29,33-34. They also reflected on how these advertising techniques normalized tobacco and e- cigarette use, enticed non-smokers to initiate smoking despite awareness of the health consequences, and have had exploitative tendencies towards vulnerable communities that face disproportionate social and economic hardships31,35,37,39.
Navigating social pressures also emerged as another prominent theme across all studies. Adolescents and young adults reported that photovoice helped them process how smoking has been normalized as a social activity, a method to gain status and assimilate into peer groups, and a way to be perceived as ‘cool’32,34,38,40. Additionally, adult participants indicated that smoking was often used as a coping mechanism for work and life stressors and that these habitual patterns often hindered cessation plans35-36. Despite these social pressures, both adolescents and adults described how photovoice helped them articulate the shame, discomfort, and judgment that smokers faced from being stigmatized in their communities30,35,40.
While participants examined marketing and social pressures related to smoking behaviors, photovoice implementation fostered collective empowerment and connection across all studies. Through shared-decision making in project design and dissemination, participants enhanced their collective awareness of smoking behaviors and strengthened prevention efforts29,31-34,37,39. The studies based on CBPR methodology also acknowledged that positioning participants as co-researchers strengthened authenticity, voice, and collaboration throughout the entire research process29,32-33,37,39. Participants also developed community solidarity that stemmed from the enriching discussion sessions and drove connections beyond the research projects31-33. This sense of community also inspired participants to advocate for tobacco and smoking prevention and partake in long-term awareness campaigns within their communities29,32,36-37,39.
Behavioral and policy outcomes from photovoice implementation
Only a few photovoice activities resulted in behavioral or policy changes. Some policies, such as a tobacco ban or retailer permit, were established because of the photovoice activity29,39. Other changes include smoking rates and indoor exposure to cigarette smoke decreasing, and health literacy scores increasing34. Advisory councils were also created because of the photovoice activity to help with policy advising37. One behavioral change mentioned was moving ashtrays to more than 25 feet from buildings38. The other articles did not have any policy or behavioral changes as their main goals were to inform and understand the role of photovoice on smoking habits30-33,35-36,40.
Final deliverables and presentations of photovoice projects
Due to differences in study design and aim, a variety of approaches were used as final deliverables of the photovoice activities. For instance, some researchers used digital media to convey the consequences of participants’ smoking behaviors29,31, while others displayed the photos at exhibitions or galleries29,33-34,37-38. Participants also presented their findings at conferences29,33 or produced physical media such as booklets32. Only one article had a final deliverable of the photos being showcased in a coalition39. However, a few studies did not clarify if a final presentation was done30,35-36,40. Of the articles that reported over a hundred photos taken and had a deliverable to show the photos34,37, not all the photos were showcased. For one article, 20 photos were used in the exhibition, but researchers did not provide specific details on the criteria or process used for their selection34.
In another article, youth participants selected their favorite photos through a consensus process, identifying 62 meaningful photos initially, then narrowing them down to their top 25 that were showcased in a gallery37. Despite our review consisting of different methods of delivery, two articles did not report how many photos were used29,33, while one article reported having 30 photos included in the exhibition38. For digital media usage, one article reported an average of 17 photos posted per participant31.The remaining articles did not report how many photos were used32,39.
DISCUSSION
Our review demonstrates that studies that integrate photovoice within smoking prevention and cessation research not only benefit participants by deepening their understanding of the social and environmental smoking influences, but also facilitate collective empowerment and support healthier behavioral choices like joining cessation programs37. This scoping review supports that photovoice represents a promising research method for meaningfully engaging diverse populations in addressing targeted marketing and sociocultural determinants of tobacco and e-cigarette smoking.
There are various ways to discuss and disseminate findings from photovoice activities41. We denoted methodological variation in achieving the second photovoice goal defined by Wang and Burris22 regarding meaningful discussion of the photos taken, as only three studies explicitly described their participants partaking in active and sustained group discussions29,33,37, in spite of six articles implementing the SHOWeD technique29,31,37-40. This heterogeneity in goal achievement limits the depth of community engagement and may account for limited impact from dissemination as well. Additionally, we found heterogeneity in the final deliverables from the photovoice activities. In most studies explored, researchers displayed the photos at art galleries, exhibitions, and conferences29,33-34,37-38. In addition, some investigators chose to create physical media to share the images or demonstrate the findings in a coalition. Thus, the diversity in sharing the findings can be beneficial to reach different audiences. Despite various options for disseminating photovoice activity findings to the public, some studies did not report any public dissemination30,35,36,40. Therefore, how well the public would have received these methods is not known. Because of this, there is a need to better examine ways to publicize photovoice activities. One example is the use of social media as digital media becomes popularized. The study by Hanby et al.31, which used Facebook and Instagram groups, was highly liked and accepted by participants. Therefore, adopting social media in photovoice-based smoking prevention research can be beneficial in reducing smoking prevalence through expansion of cessation programs.
Our review shows that participants receive training on how to carry out the photovoice activities, which involve taking photos around their communities. We found differences in methods of capturing photos, data analysis, and ethical implications. While some researchers provided participants with digital cameras or disposable cameras30,32,35-38,40, others had participants use their cellular devices29,35. There is no evidence that states which device is the best to carry out a photovoice method, allowing researchers and participants to decide which method would be easiest to convey the message42. Coupled with this training, the majority of the researchers showcased were briefed on ethical considerations and received feedback on how to improve ethical guidance for photovoice. For example, in one article, researchers encountered unfriendliness and racially based aggression from store employees, highlighting the need for safety planning integrated into Institutional Review Board protocols for future CBPR studies29. Because of this, we recommend that future research establish comprehensive ethical best practices for photovoice work with different populations. Many of the researchers also informed the participants of the SHOWed method29,31,37-40, emphasizing the effectiveness of describing the photographs and extracting data from it. Even the researchers who did not specify a method incorporate parts of the SHOWed method in their analysis. These similarities will be useful for designing future photovoice studies on smoking behavior and advocating for smoking cessation programs.
Our review shows that the photovoice activities can lead to policy and behavioral changes regarding smoking, such as tobacco bans, retailer permits29,39, and making ashtrays more inaccessible38. In addition to this, photovoice activities can inform community members of the effects of tobacco use and improve their health literacy. Additionally, these specific studies have populations that were mostly underserved, and the photovoice activity resulted in positive feedback31, reduced smoking34, empowerment of youth29,39, increased awareness32, and increased cessation program attendance37 within these specific communities. Utilizing what worked in these studies can be applicable on a larger scale to address smoking disparities for marginalized communities nationwide43.
Strengths and limitations
Our scoping review addresses a gap in smoking control literature by systematically synthesizing the use of photovoice in tobacco and vaping prevention and cessation research. It provides a timely and comprehensive overview of how photovoice has been leveraged in smoking prevention and cessation by analyzing studies published since 2010 with particular attention on the impact on youth and young adults, who remain primary targets of tobacco and e-cigarette marketing. Additionally, the review highlights the versatility of photovoice in tobacco control research by examining its use across schools, universities, and CBPR-based initiatives, which enables a stronger evaluation of the methodological flexibility and adaptability of photovoice in diverse settings29,32-35,37-39. Thus, the findings reported offer a foundation for designing photovoice-centered studies in tobacco smoking and e-cigarette control research and for strengthening their methodological rigor and impact on prevention and cessation outcomes and policy reform.
The study has some limitations. Although we conducted a comprehensive review of photovoice studies, restricting inclusion to only journal articles published in English may have limited the generalizability. Heterogeneity in participant demographics, study designs, photovoice training method duration and implementation, and dissemination strategies reduced the ability to assess comparability across findings and limited the generalizability of reported outcomes across diverse populations. Inconsistent age reporting hindered the ability to evaluate the impact of photovoice across developmental stages and its influence on smoking as a modifiable behavioral factor, which is often linked to chronic disease risk. Similarly, variation in reported smoking status (non-smoker, smoker, recently quit) at the time of recruitment complicated efforts to evaluate the direct role of photovoice in smoking reduction and cessation. Only Haines-Saah et al.30 targeted recent quitters attempting cessation, while four did not report participants’ smoking status29,33,37-38, making it difficult to distinguish the effects of photovoice from existing prevention and cessation services.
Additionally, the use of photovoice in vaping prevention and cessation remains limited, with Chopel et al.29 as the sole study in our review examining this intersection despite the predominant smoking mechanism used by youth and young adults44. Variation in photovoice training method durations further complicated efforts to identify optimal parameters for successful outcomes and sustained impact. These variations also made extraction difficult to report heterogeneously, resulting in our table having a descriptive format. Additionally, the lack of standardized outcomes measured for health education, awareness, and empowerment across the studies limited comparative assessments of photovoice effectiveness. Finally, causality could not be determined from our work due to heterogeneous outcomes reported, the predominance of qualitative metrics, and the exclusion of the grey literature.
Quality assessment was not conducted for this review due to the heterogeneity in photovoice methodology and implementation. Furthermore, variable reporting on the sustainability of community activism and advocacy efforts post-photovoice implementation from both articles partially, fully, and not immersed in CBPR framework limits understanding of the long-term community level impacts of photovoice. The absence of longitudinal data with these studies restricts ability to evaluate sustained behavior change and continued community engagement beyond intervention periods. Future research should differentiate effects of photovoice from traditional interventions and health promotion programs and understand the unique contributions to smoking behavior change. Incorporating consistent measures of health education and health literacy will also better tailor interventions for marginalized communities.
CONCLUSIONS
Leveraging photovoice as a research method for smoking prevention and cessation has provided community members with greater understanding on the various influences and pressures associated with smoking behaviors as well as the barriers that prevent uptake of cessation services. Photovoice has offered a creative avenue for tobacco and e-cigarette education by incorporating participants at all stages of the research process, building trust in community-based participatory research from active engagement, and strengthening reflection on the impact of these services within their communities through participant documentation on environmental impacts from smoking. Further investigation of applying photovoice in smoking cessation research could help us to better structure and tailor culturally competent programs for marginalized populations and reduce prevalence of a major chronic disease risk factor.