INTRODUCTION
The tobacco epidemic kills more than 8 million people worldwide each year and is one of the biggest public health threats the world has faced. More than 7 million of these deaths are the result of direct tobacco use and around 1.2 million are the result of non-smokers being exposed to secondhand smoke1. In this context, clarifying the factors associated with smoking behaviors may be useful to determine appropriate interventions to promote smoking cessation. Numerous previous studies investigated factors associated with smoking behaviors including smoking status2,3, smoking initiation4,5, smoking cessation6-8, and smoking relapse9,10. In addition, previous systematic reviews grouped these factors into conceptually similar categories11-16, such as social, environmental, and individual factors11. Recently, health literacy has been revealed as an important factor associated with smoking-related behaviors or issues17-20.
The concept of health literacy was initially introduced during the 1970s and defined as the ability to read, understand, evaluate, and use health information necessary to make reasoned, health-related decisions21. In the last few decades, there has been an extraordinary growth in interest in health literacy worldwide in both healthcare and in the public health context22,23. Furthermore, a new and more detailed definition of health literacy is linked to literacy and entails people’s knowledge, motivation, and competence to access, understand, appraise, and apply health information to make judgments and decisions in everyday life concerning healthcare, disease prevention, and health promotion to maintain or improve quality of life during the life course24. In addition, several health literacy assessment instruments have been developed and validated, including the Rapid Estimate of Adult Literacy in Medicine (REALM)25, the Test of Functional Health Literacy in Adults (TOFHLA)26, and the Newest Vial Sign (NVS)27. In addition to general health literacy, other contexts such as eHealth literacy28,29, mental health literacy30, media health literacy31, and nutrition literacy32, are being discussed.
Previous literature reviews have reported associations between health literacy and various important issues such as health disparities33, women’s reproductive health34, cancer prevention35, and adherence to medication36. However, no literature reviews have synthesized the associations between health literacy and smoking-related behaviors or issues. Therefore, this review aimed to assess the associations between health literacy and smoking-related behaviors or issues.
METHODS
Search strategy
We searched published literature in four electronic databases (PubMed, CINAHL Plus, Scopus, and Web of Science) from inception to 22 February 2021. The search was limited to articles written in English and published in scientific journals. We used combinations of key words, including health literacy, tobacco, smoking, nicotine, cigarettes, vaping, e-cig, and e-cigarette. Detailed search strategies are presented in the Supplementary file. The reference lists of identified articles and Google Scholar were also manually searched.
Data extraction
We extracted the following data including author/year, country, study design, study subject (sex, age, number of participants), health literacy assessment instruments, smoking-related behaviors or issues, multivariate analysis, and associations between health literacy and smoking. The first author (ML) independently identified relevant studies, and a data collection sheet (Supplementary file) designed by two authors (AM and ML) was used to summarize the extracted data. The extracted data were checked for accuracy by all authors.
Inclusion and exclusion criteria
Eligibility criteria were defined prior to the database search in order to only include studies that were relevant to the research question. The inclusion criteria were: 1) articles written in English, 2) articles published in scientific journals, 3) quantitative studies, and 4) studies examining the associations between health literacy and smoking-related behaviors or issues. We excluded articles that did not meet the inclusion criteria.
Meta-analysis
The extracted data regarding the association between health literacy and smoking was subjected to meta-analysis using Review Manager software (Review Manager, version 5.4.1, The Cochrane Collaboration, Oxford, England). The results of meta-analysis are reported as a weighted odds ratios (ORs) with 95% confidence interval (CI). The Cochrane chi-squared (Q) test was used to assess heterogeneity among studies, with p≤0.1 indicating the existence of heterogeneity, and I2 value was used to estimate the impact of heterogeneity on the meta-analysis. Heterogeneity was regarded as: none (I2<25%), low (25%≤I2<50%), moderate (25%≤I2<75%), or high (I2≥75%). In the presence of moderate or high heterogeneity (I2>50%), the random-effects model was used, while if none or low heterogeneity was found (I2<50%), the fixed-effects model was used. For forest plots with the included sufficient studies (>10 articles), funnel plots were generated to examine for the publication bias.
In the meta-analysis, we defined smoker, current, daily, occasional and regular smoker, people who smoke every day or some days, people with tobacco use, and people with cigarette and hookah use as smokers, and the rest of the population (non-smoker, former, never, not daily, not current, and not regular smoker, people who did not smoke at all, people with no tobacco use, and people with no cigarette and hookah use) as non-smokers. Additionally, for health literacy, we defined adequate, high, higher, sufficient and ≥9th grade of REALM in the included study as adequate health literacy group, and the rest (limited, low, at-risk, inadequate, problematic, marginal, medium, borderline, 0 to 8th grade of REALM, and very limited) as inadequate health literacy group, although different health literacy assessment tools were used in different studies.
RESULTS
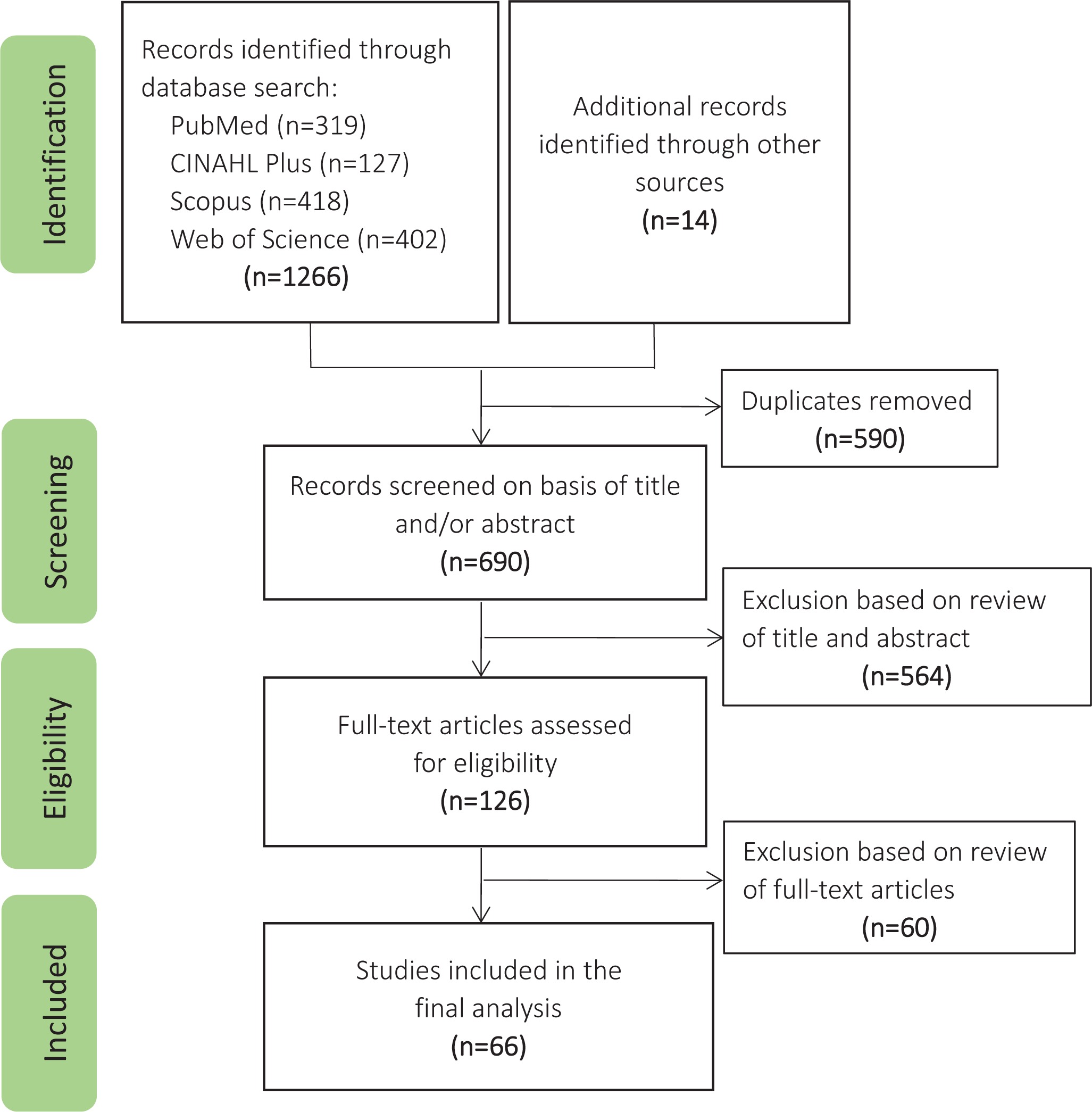
The initial database search yielded 1266 articles. A further 14 articles were obtained through a manual search. After excluding 590 duplicate articles (automatically excluded by EndNote software: n=296; manually excluded: n=294), 690 articles remained for title and abstract screening. Of these, 564 articles were excluded and the remaining 126 articles underwent full-text screening. We excluded 60 articles that were not relevant to the associations between health literacy and smoking-related behaviors or issues. Finally, 66 articles were included in the present analysis17-20,37-98 (Figure 1).
Figure 1
Flow chart of articles identified within this meta-analysis of the association between health literacy and smoking
Characteristics of the included studies
Characteristics of the included studies are summarized in the Supplementary file. The 66 included articles included 23 articles from America19,20,39,42,43-45,52,53,60-62,73-76,82,83,85,93-95,98, five from Iran18,77,78,80,81, five from Denmark37,54,55,66,87, four from Japan58,84,86,88, three from Turkey48,96,97, three from the Netherlands56,63,89, three from China70-72, three from Australia38,59,64, two from Taiwan51,67, two from the UK17,91, two from Ghana40,41, and one each from Germany46, Switzerland49, Vietnam50, Spain90, Korea68, Kazakhstan65, Jordan79, Israel69, Ireland57, Greece92, and Austria47.
Most included studies used cross-sectional designs or were cross-sectional analyses using baseline data from a longitudinal study or randomized controlled trial. The measures most commonly used to assess the association between health literacy and smoking-related behaviors or issues were the NVS38,53,74,86,90,96, REALM20,42,76,82,83,85,97, TOFHLA39,43-45,52,60-62,76,80,91,93,94, the European Health Literacy Survey Questionnaire (HLS-EU-Q)41,47,51,57,65,69,87, and the Health Literacy Questionnaire (HLQ)54,55,79,81. In addition, health literacy assessment instruments in various languages were used to assess the association between health literacy and smoking-related behaviors or issues, such as the 14-item health literacy scale for Japanese adults and Communicative and Critical Health Literacy in Japan58,86, Chinese Citizen Health Literacy Questionnaire in China71,72, and Korean Health Literacy Instrument in Korea68.
Association between health literacy and smoking
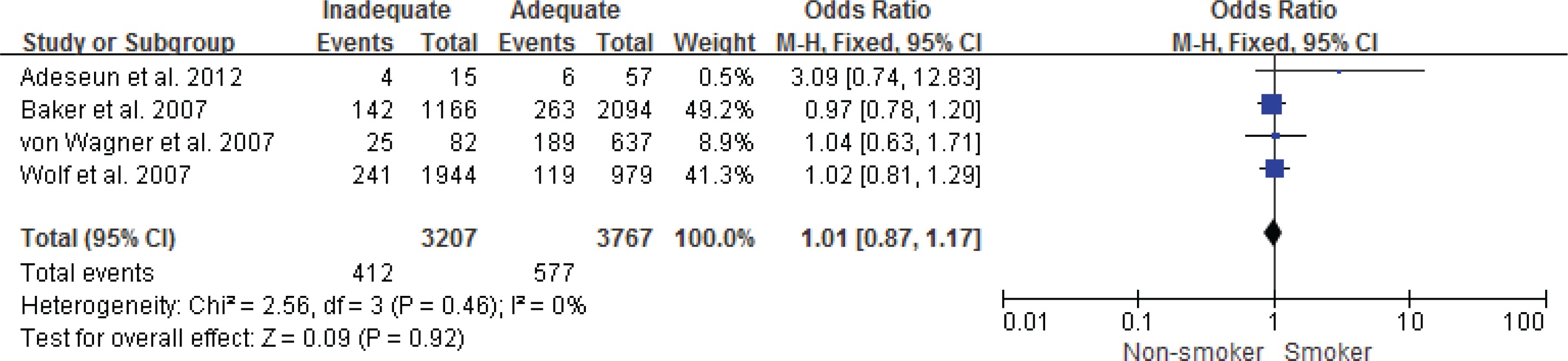
Figure 2 shows the pooled OR with 95% CI for smoker according to inadequate and adequate groups of health literacy, the pooled OR (95% CI) for smoker was 1.49 (1.25– 1.79) in the inadequate health literacy group, compared with the adequate health literacy group. There was a high heterogeneity among the included 22 studies (p<0.001, I2=80%). The visual inspection of the funnel plot showed no symmetry, which indicated evidence of publication bias (Figure 3). Additionally, with health literacy assessed by NVS, REALM and TOFHLA, the pooled ORs (95% CIs) for smoker were: 1.37 (95% CI: 0.94–2.01, I2=62%, three studies) (Figure 4), 1.25 (95% CI: 0.67–2.34, I2=77%, three studies) (Figure 5), and 1.01 (95% CI: 0.87–1.17, I2=0%, four studies) (Figure 6) in the inadequate health literacy group, compared with the adequate health literacy group, respectively.
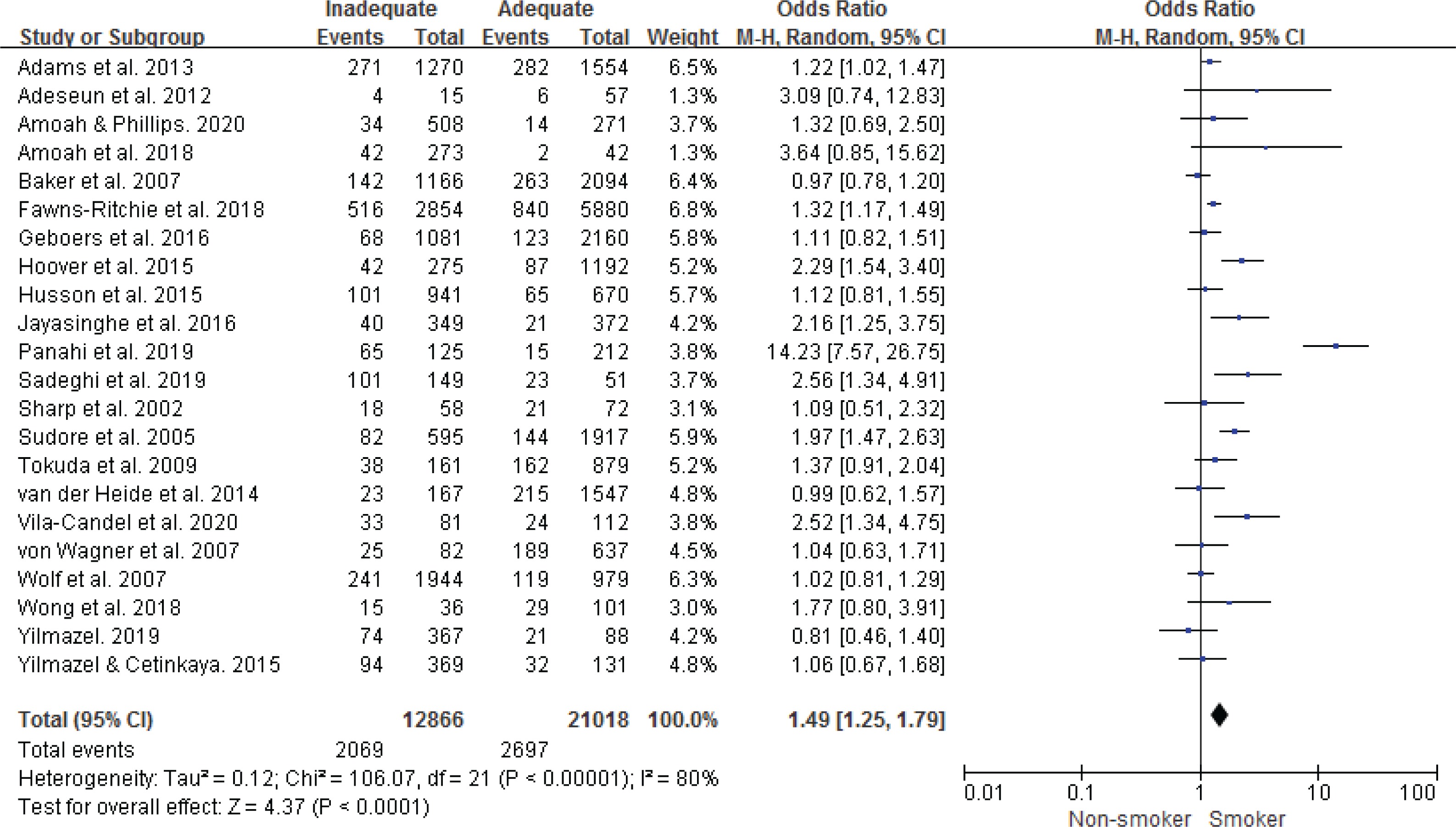
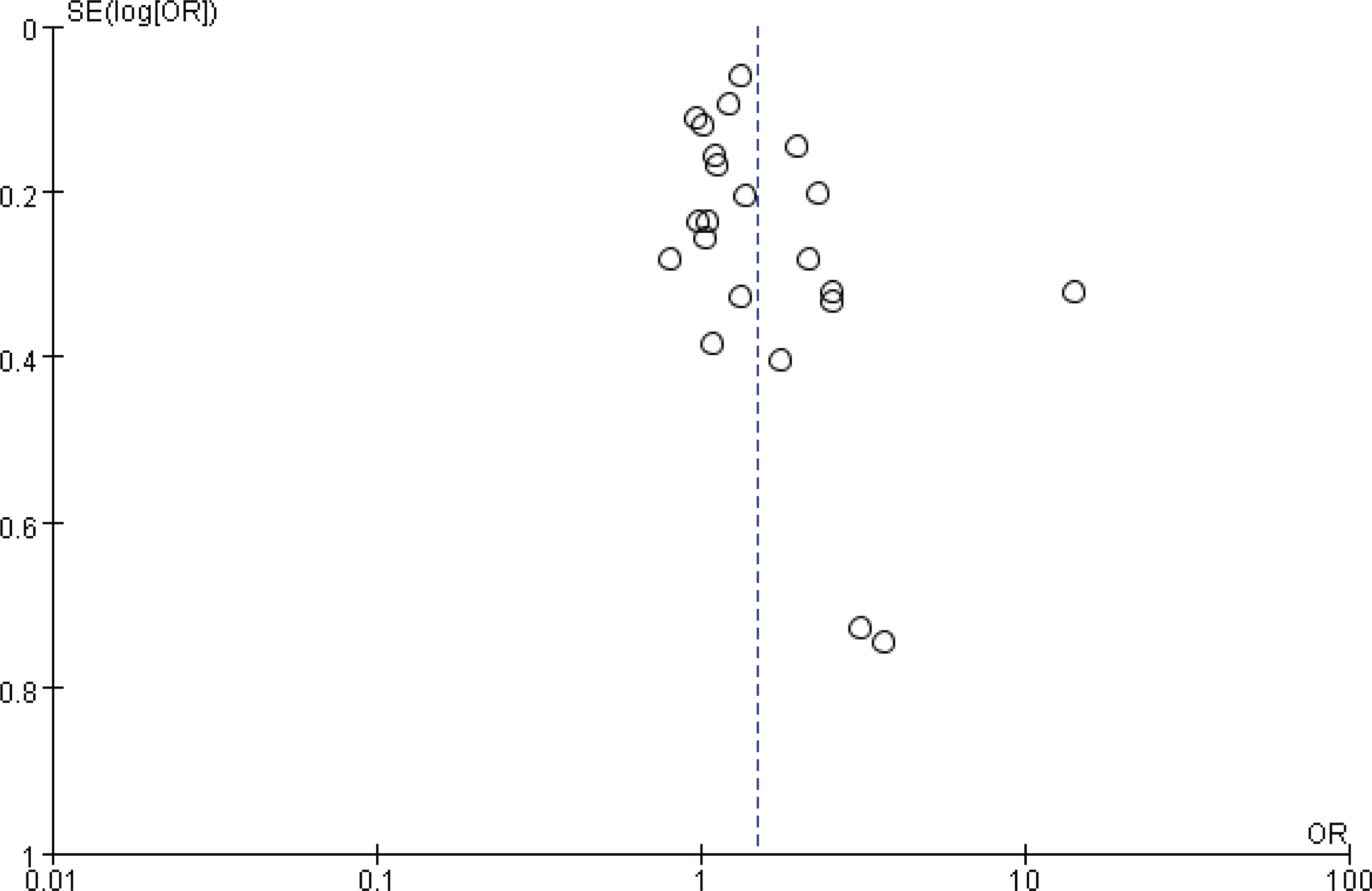
Figure 4
Forest plot of the meta-analysis of the association between smoking and health literacy assessed by NVS

Figure 5
Forest plot of the meta-analysis of the association between smoking and health literacy assessed by REALM
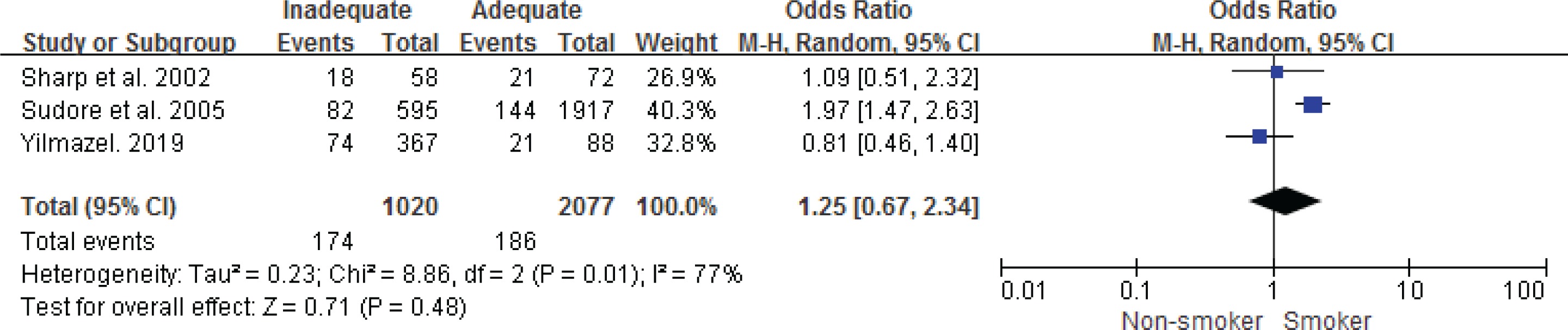
Figure 6
Forest plot of the meta-analysis of the association between smoking and health literacy assessed by TOFHLA
Moreover, previous studies also reported that inadequate health literacy was significantly positively associated with a high possibility of current smoking compared with former smoking in those that had ever smoked17 and smoking relapse83, and a low possibility of smoking cessation18,75. A previous cohort study from the Netherlands reported that inadequate health literacy was not associated with smoking; however, the association between health literacy and smoking was moderated by social contacts56.
Association between health literacy and smoking-related issues
Many studies reported that health literacy was significantly associated with other smoking-related issues such as knowledge about the effects of smoking, nicotine dependence, expectations for quitting, susceptibility to future smoking, and uptake of smoking cessation aids20,42,46,60,84. In addition, two studies conducted in the US and China reported associations between e-cigarette health literacy and e-cigarette use-related behaviors, such as perceived benefits and risks of e-cigarette use, attitude towards e-cigarettes, disengagement belief, and e-cigarette susceptibility70,98.
DISCUSSION
We assessed the associations between health literacy and smoking-related behaviors or issues. The meta-analysis among the included 22 studies showed that the pooled OR (95% CI) for smoker was 1.49 (95% CI: 1.25–1.79) in the inadequate health literacy group, compared with the adequate health literacy group. Moreover, previous studies reported that inadequate health literacy was significantly positively associated with a high possibility of current smoking compared with former smoking in those that had ever smoked17 and smoking relapse83, and a low possibility of smoking cessation18,75.
There were three important points that warrant discussion. First, the meta-analysis among the included 22 studies revealed that those with inadequate health literacy was 1.49 times more likely to be a smoker, compared with the adequate health literacy. Of these, Hoover et al.19 reported that inadequate health literacy was significantly associated with current smoking compared with never smoking among African American adults in the US. Amoah and Phillips41 reported that among rural and urban residents in Ghana, daily smokers and occasional smokers were likely to have sufficient health literacy compared with never smokers. In addition, Gibney et al.57 reported that for the low and middle social status groups, adequate health literacy was associated with a lower probability of being a current smoker. VilaCandel et al.90 reported among women in Spain, inadequate health literacy was strongly associated with tobacco use during pregnancy. These findings suggested improving health literacy may help prevent smoking.
Regarding the reasons why inadequate health literacy was significantly positively associated with a high possibility of smoking, Adams et al.38 reported that people in Australia who perceived smoking to be not important or did not know if there were important cancer risks were more likely to have inadequate functional health literacy. In addition, Sudo and Kuroda84 reported that interactive health literacy was negatively associated with susceptibility to future smoking among adolescents in Japan. These findings suggest that those with inadequate health literacy were more likely to be in the smoker group compared with those with adequate health literacy.
Second, previous study reported that inadequate health literacy was significantly positively associated with a high possibility of current smoking compared with former smoking among those that had ever smoked among ever smokers aged ≥50 years in England17. Similarly, a recent study in Japan reported that inadequate health literacy was positively associated with current smoking compared with former smoking among middle-aged Japanese ever smokers99. Regarding reasons why smokers with inadequate health literacy were less likely to quit smoking, Stewart et al. 10 reported that in America, inadequate health literacy was significantly associated with having high nicotine dependence, more positive smoking outcome expectancy (e.g. social facilitation), less negative smoking outcome expectancy (e.g. health risks), less knowledge about smoking health risks, and low risk perceptions.
Conversely, improving health literacy may promote smokers to quit smoking. Martin et al.75 reported that among regular smokers in the US, the odds of quitting smoking increased by about 8% for each grade equivalent increase in reading skills, and the odds of quitting increased by about 24% for every point increase in numeracy skills. Atri et al.18 found a significant, positive relationship between health literacy and the stages of behavior change among employees in educational and medical centers of Tabriz. By improving health literacy, people can be helped to change their behavior from the precontemplation stage to the continuation and maintenance stages.
In addition, Stewart et al.83 reported that smokers in the US with inadequate health literacy were more likely to relapse by the end of smoking cessation treatment compared with those with adequate health literacy. The result suggests that improving health literacy may avoid smoking relapse. Regarding methods to improve health literacy, a randomized controlled trial indicated in a Japanese rural community, health education through a weekly 90-minute active learning program including exploratory learning, group work, and self-planning for behavioral change was effective in enhancing comprehensive health literacy in older adults100.
Third, our results indicate that the most commonly used measures to assess the association between health literacy and smoking were the NVS38,53,74,86,90,96, REALM20,42,76,82,83,85,97, TOFHLA39,43–45,52,60–62,76,80,91,93,94, HLS-EU-Q41,47,51,57,65,69,87, and HLQ51,55,79,81. However, in the meta-analysis to assess the associations between smoking and health literacy assessed by NVS, REALM and TOFHLA, they were not significant. Meanwhile, considering the content of these scales101,102, we think that these scales may not be appropriate for measuring smoking-related health literacy. In recent years, many health literacy scales are available that are classified by various diseases or conditions, such as the Diabetes Health Literacy Scale103, Cancer Health Literacy Scale104, and Health Literacy in Dentistry105. Therefore, a specific smoking-related health literacy scale may be needed.
Limitations
This study had some limitations. First, our search only identified articles published in English and in selected databases. Thus, this study might have missed other studies that were published in other languages and in other databases. Second, we redefined the group of health literacy and smoking status for the meta-analysis according to our consideration and may affect the accuracy of the results. Third, most included studies used cross-sectional designs or were cross-sectional analyses. Thus, the associations between health literacy and smoking-related behaviors or issues could not be adequately demonstrated.
CONCLUSIONS
The meta-analysis among the included 22 studies revealed that those with inadequate health literacy were more likely to be smokers, compared with the adequate health literacy. Moreover, previous studies reported that inadequate health literacy was significantly positively associated with a high possibility of current smoking compared with former smoking in those that had ever smoked and smoking relapse, and a low possibility of smoking cessation. Improving health literacy may be useful to prevent smoking, promote smoking cessation, and avoid smoking relapse.