

INTRODUCTION
Mental health is an important aspect of adolescent development. This period is a transitional phase characterized by very rapid biological, psychological, and social changes that make it susceptible to the emergence of various mental health problems1-3. The World Health Organization (WHO) confirms that around 1 in 7 adolescents in the world experience mental disorders, including depression2. Depression in adolescence is one of the most impactful health problems, as it is associated with poorer academic and social functioning in the future, which suggests that the impact of depression on adolescence can extend far beyond the adolescent period itself4,5.
The burden of mental health problems in adolescents in Indonesia also shows a tendency that needs attention. I-NAMHS reports that about 1 in 3 adolescents (34.9%) have mental health problems, and about 1 in 20 adolescents (5.5%) have met the criteria for a mental disorder6. In addition, I-NAMHS also showed that the prevalence of depression in female adolescents (6.7%) was higher than that of adolescent boys (4.0%), which indicates a gender-based vulnerability to adolescent mental health problems6. In line with that, the 2023 Indonesian Health Survey (SKI) reported that the national prevalence of depression was 1.4%, with the highest proportion of 2.0% found in the age group of 15–24 years7. In this young age group, the prevalence of depression in women (2.8%) is also higher than in men (1.1%), which further confirms that female adolescents are a more vulnerable group to depression7.
Previous research related to depression in Indonesia has found that sociodemographic factors, including gender, marital status, location of residence, and behavioral factors such as smoking, contribute to depression in adolescents8,9. Previous research has shown that female adolescents have a higher risk of depression than adolescent boys8. In line with these findings, this study aims to determine the prevalence of depression and factors associated with it in female adolescents aged 15–19 years in Indonesia using the 2023 SKI Survey.
METHODS
Study design and data source
We conducted a secondary dataset analysis of the cross-sectional Indonesian Health Survey 2023. This data collection was conducted nationwide by the National Development Planning Agency (BKPK) from August to October 2023, covering 38 provinces and 514 districts/cities in Indonesia. Therefore, these data can represent the health status at the national to district/city level7.
Participants
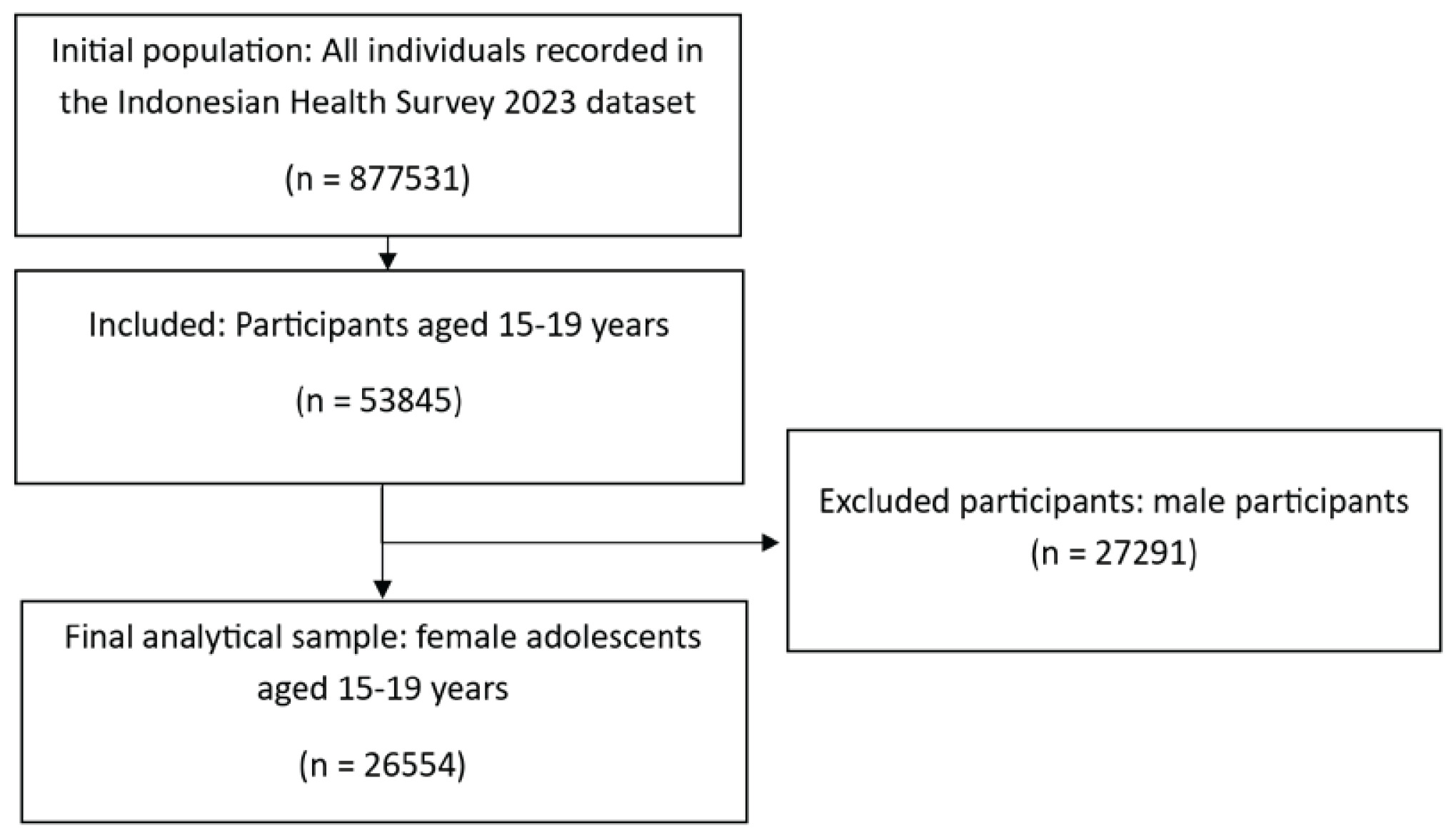
The Indonesian Health Survey covered the entire territory of Indonesia, recording 1082958 household members, of whom with 877531 individuals completed the interview and measurement process7. In this study, participants for analysis were selected from the 2023 SKI individual data set using the inclusion criterion of being aged 15–19 years. After selection, 53845 respondents met these criteria. A total of 27291 male respondents were excluded from the analysis, leaving a final analytical sample that consisted of 26554 female adolescents aged 15–19 years in Indonesia (Figure 1).
Data collection
Data collection in the 2023 Indonesian Health Survey was conducted through interviews, measurements, and examinations. For regular households, the interview component used two instruments, namely the household questionnaire and the individual questionnaire. The dependent and independent variables analyzed in this study were obtained from the individual questionnaire in Block XI, which consists of Blocks A to J. The independent variable, smoking status, was derived from Block G, which covers knowledge and behavior. The dependent variable, depression, was obtained from Block C, which addresses mental health. Finally, covariates such as employment status, marital status, education level, and location of residence were obtained from the household questionnaire, specifically from Block IV (Household Member Information) and Block I (Location Identification)7 (Supplementary file).
Variables
Dependent variable
This study defines depression as a dependent variable. The depression variable was assessed using the Mini International Neuropsychiatric Interview (MINI) instrument, referring to symptoms experienced during the previous two weeks. The instrument consists of 10 questions with ‘yes’ or ‘no’ responses. Examples of the items include questions about persistent sadness over the previous two weeks, diminished interest or enjoyment in usual activities, and ongoing feelings of tiredness or low energy. Respondents were considered to have depression if they answered ‘yes’ to at least 2 of the 3 main questions (questions 1–3) and also ‘yes’ to at least 2 of the 7 additional questions (questions 4–10)10.
Independent variable
Smoking status was defined as an independent variable in this study and classified into three categories: never smoker, ex-smoker, and current smoker. Respondents were categorized as never smokers if they had never tried smoking until the time of data collection. The ex-smoker category referred to respondents who had smoked previously, either daily or occasionally, but not on a daily basis at the time of assessment. Meanwhile, respondents were classified as current smokers if they had smoked every day or occasionally during the past month7.
Covariates
Covariates in this study included employment status, marital status, education level, and location of residence. Employment status was categorized as either employed or not employed. Marital status was classified as never married, married, or divorced/widowed. Education level was determined based on the highest level of formal education completed and grouped into at least high school education and lower than high school education. Location of residence was defined according to the village/urban ward classification and categorized as either urban or rural.
Covariates were selected based on prior literature indicating that these variables may be associated with depression8,9,11,12. Therefore, they were considered important for adjustment in the multivariable analysis using a determinant modeling approach, in which all variables were assumed to have an equal opportunity to influence the occurrence of depression. The selection of these covariates was based on Lawrence Green’s theory.
Data management and statistical analysis
The data management process began with extracting relevant variables from the 2023 Indonesian Health Survey database. Data cleaning was carried out to identify missing values and ensure logical consistency between sociodemographic variables and mental health instrument scores. The dependent variable, namely depression, was dichotomized using the Mini International Neuropsychiatric Interview (MINI) instrument at the cutoff point. Independent variables such as smoking status, age group, education level, employment status, marital status, and location of residence (urban, rural) were recoded to facilitate interpretation. The entire data processing process integrated weighting variables, strata, and primary sampling units (PSUs) to compensate for the complex survey design, enabling the estimation results to be generalized to the national population of female adolescents in Indonesia.
Data analysis was conducted in stages using an inferential statistical approach. Univariate analysis was used to describe the frequency distributions of respondents’ characteristics, with percentages reported for categorical variables and means ± standard deviations (SD) for continuous variables. Bivariate analysis was performed to test the relationship between the independent variables and depression using the chi-squared test, accounting for the survey design. Furthermore, multivariate analysis was performed using multiple logistic regression to identify the most influential determinants of depression in female adolescents, after controlling for covariates. The results of the multivariate analysis were presented as crude odds ratios (OR) and adjusted odds ratios (AOR) with 95% confidence intervals. All statistical procedures were performed using software that supports the complex-samples module to ensure accurate standard error estimates.
Ethical aspects
This study is a further analysis using secondary data from the 2023 Indonesian Health Survey (SKI). The survey protocol has been declared ethically sound by the Formal Health Research Ethics Commission of the Health Development Policy Agency (BKPK), Indonesian Ministry of Health, under number LB.02.01/2/KE.024/2023. All respondent identities in the dataset have been anonymized by the survey organizers to maintain the confidentiality of the research subjects.
RESULTS
Table 1 presents the distribution of sociodemographic characteristics, age of smoking initiation, smoking status, and depression among 26554 female adolescents aged 15–19 years in Indonesia. The largest age groups were aged 16 years (22.2%) and aged 15 years (21.7%), with a mean age of 17.14 ± 1.34 years. Most participants had lower than a high school education (79.2%). The majority were employed (74.1%), while 25.9% were not employed. Most female adolescents had never been married (95.9%), followed by those who were married (3.9%) and divorced/widowed (0.2%). Based on the location of residence, more participants lived in urban areas (57.8%) than in rural areas (42.2%). The mean age of smoking initiation was 15.48 ± 2.08 years. Most participants had never smoked (99.4%), while 0.4% reported being ex-smokers and 0.2% reported being current smokers. The prevalence of depression in this study was 1.6% among female adolescents aged 15–19 years in Indonesia.
Table 1
Sociodemographic characteristics, age of smoking initiation, smoking status, and depressive symptoms among female adolescents aged 15–19 years in Indonesia, based on SKI 2023 (N=26554)
The prevalence of depression was higher among ex-smokers (27,4%), followed by current smokers (18,9%). Bivariate analysis with chi-squared test showed a significant association between smoking status and depression (p=0.001) at 95% confidence. Further analysis with a simple logistic regression test showed that female adolescents who were past smokers were 12.59 times more likely (95% CI: 12.37–12.82) to experience depression than adolescents who were never smokers. Female adolescents who are current smokers have an 8.10 times greater chance (95% CI: 7.79–8.43) than female adolescents who were never smokers (Table 2).
Table 2
Bivariate analysis of smoking status and depressive symptoms using chi-squared test among female adolescents aged 15–19 years, based on SKI 2023 (N=26554)
The results of multivariate modeling showed that female adolescents who were ex-smokers were 10.93 times more likely (95% CI: 10.73–11.13) to experience depression compared to female adolescents who were never smokers. Meanwhile, female adolescents who are current smokers are 5.82 times more likely (95% CI 5.58–6.08) to experience depression compared to those who were never smokers. Further results were also obtained that divorced female adolescents were 4.32 times more likely (95% CI: 4.15–4.49) to experience depression than unmarried women. Female adolescents living in urban areas were 2.12 times more likely (95% CI: 2.10–2.13) to experience depression than those living in rural areas (Table 3).
Table 3
Adjusted prevalence odds ratios (AOR) for depressive symptoms by smoking status and sociodemographic covariates among female adolescents aged 15–19 years, SKI 2023 (N=26554)
DISCUSSION
This study identified that the prevalence of depression is 1.6% among older female adolescents in Indonesia. This prevalence is lower than that of other national surveys in Indonesia. One study reported a prevalence of 6.7% for female adolescents aged 10–17 years6. Research in Indonesia using the Indonesia Family Life Survey data on female adolescents aged 15–19 years also showed much higher results, namely 26.3%, compared to those who were not depressed9. The differences in findings across prevalence rates can be influenced by differences in study design, variation in study populations, and the definition or instrument used to assess depression.
Important findings in this study show that there is a relationship between smoking status, marital status, location of residence, and depression in female adolescents, which is consistent with previous research8,9. This finding is in line with Lawrence Green’s theory that the incidence of depression in female adolescents can be influenced by the interaction of various determinants, including predisposing factors, enabling factors, and reinforcing factors.
The findings of our study reinforce previous evidence showing a link between smoking status and depression in female adolescents10,11. In line with that, a study in Indonesia on female adolescents aged 15–19 years also identified smoking status as one of the factors related to common mental disorders12. This relationship is thought to be related to nicotine exposure13,14. Recent studies have shown that the association between nicotine exposure and depressive symptoms is more meaningful in women with increased depressive symptoms at certain nicotine exposure levels13. In addition, it is thought that active maturation of the acetylcholine and dopamine systems that play a role in the regulation of mood, affect, and cognitive control in adolescents may be disrupted in their development by nicotine exposure associated with susceptibility to mental health disorders, including depression14,15. In line with this, previous studies have found that a younger age of first exposure to cigarettes is associated with an increased risk of major depressive episodes16,17.
In our analysis, ex-smokers were at a higher risk for depression than those who were never smokers, and the risk was even higher than that of current smokers. Research in Indonesia on adolescents and young adults is also in line with these results8,9. Consistent with this, a national study in the US found that ex-smokers were also associated with a higher risk of depression than non-smokers, but the amount of risk was no greater than that of current smokers18. In line with the study, the association between ex-smokers and depressive symptoms is likely to be higher in females; other factors, such as having recently quit smoking, having a history of high cumulative exposure, and former dual users, are also suspected to be related19. In women, the high risk of depression in ex-smokers is thought to be related to nicotine withdrawal symptoms that are influenced by fluctuations in ovarian hormones throughout the menstrual cycle20. However, given the cross-sectional design of this study, the direction of this relationship is uncertain, and there is a possibility of reverse causality between smoking and depression.
Our study found that divorced/widowed female adolescents were 4.32 times more at risk of depression than those who had never married. These results are in line with a study in the Philippines on adolescents that reported that separation, including living divorced or widowed, was associated with a 2.02-fold increased risk of depressive symptoms compared to unmarried status21. Studies on divorced single-parent women show that there is self-stigma in divorced single-parent women, which is associated with an increased risk of mental health distress through decreased self-esteem22. These results suggest that the breakdown of marital bonds is likely accompanied by psychosocial burdens that increase vulnerability to depression.
Living in urban areas is associated with a higher risk of depression than living in rural areas in female adolescents in Indonesia. These findings are in line with previous research in Bangladesh that showed that female adolescents living in urban non-slum areas are more at risk of depression than those living in rural areas23. Similarly, a national study in South Africa reported that the prevalence of depression in adolescents living in urban areas was higher than that of rural adolescents, at 14.64% and 9.40%24. However, these findings are inconsistent with studies in Korea, which show that the proportion of moderate-severe depression symptoms is higher in rural than urban groups and confirm that the determinants of depression differ according to the context of residence25. Symptoms of depression in female adolescents living in urban areas are more associated with assessments of personal health conditions and pressure due to academic achievement demands, while in rural groups, they are related to rule violations and academic problems25. Depression in female adolescents is likely contextual, so the influence of urbanity on depression is likely mediated by social, academic, and environmental pressures that differ between countries. Further research needs to use a longitudinal design in order to better elucidate the direction of the relationship between residence and depression in female adolescents.
Strengths and limitations
This study has some strengths. This study used a large national sample of Indonesian late adolescent females. The main focus is on female adolescents aged 15–19 years, so the analysis is more specific to groups that are often overlooked in general studies of adolescents. Furthermore, the findings that smoking status is associated with depression in female adolescents in this study may strengthen the evidence of a link between smoking status and depression in these populations. There are limitations in this study that should be considered when interpreting the results. First, cross-sectional designs do not allow for causal or two-way relationships between variables. Second, this study used secondary data, so other variables that may affect depression in female adolescents could not be controlled in this study.
Implications
These findings have important implications for efforts to promote mental health in female adolescents, especially groups in more vulnerable social conditions in Indonesia. The results of the study show the need to improve early detection of depression and the development of prevention and intervention programs that are sensitive to the context of female adolescents’ development. Furthermore, longitudinal research and studies with national samples that specifically target the adolescent girl population are needed to explain the direction of stronger relationships.
CONCLUSIONS
The prevalence of depression among female adolescents aged 15–19 years in Indonesia was 1.6%. Smoking status, marital status, and location of residence were associated with depression in this population. Female adolescents who were ex-smokers and current smokers had higher odds of depression than those who were never smokers, with the highest odds observed among ex-smokers. Divorced/widowed female adolescents also had higher odds of depression than those who had never married, and those living in urban areas had higher odds of depression than those living in rural areas. These findings indicate that older female adolescents with these characteristics may represent important subgroups for depression screening and prevention efforts in Indonesia.