

INTRODUCTION
Tobacco use is one of the leading preventable risk factors associated with diseases worldwide, and it kills half of its users who do not quit1. Tobacco use leads to lung diseases, emphysema, chronic bronchitis, coronary heart disease, stroke, and at least 17 different forms of cancers2.
Currently, about 1.3 billion people smoke tobacco worldwide, resulting in more than 8 million deaths from tobacco-related complications each year, which includes approximately 1.3 million deaths from exposure to secondhand smoke3. It is estimated that tobacco use could kill one billion people this century, 70% of them in developing countries like Bangladesh4. The most common form of tobacco use in Bangladesh is smoking cigarettes. Use of smoking tobacco is relatively higher in Bangladesh (20.1%)5 compared to other South Asian countries, 20.7% in Nepal6, 18.5% in Sri Lanka7, 14.0% in India8, and 12.4% in Pakistan8.
To understand tobacco use cessation, we need a keen insight into the behavior change of smokers and their stages. Smoking cessation is a prime target for avoiding and lessening the burden of smoking-related diseases. Quitting smoking at any age has significant and immediate health benefits, such as lower odds of stroke, cardiovascular disease, and smoking-related cancers, and quitting by the age of 44 years reduces the risk of dying from tobacco-related cancer by 89%9. As a result, promoting smoking cessation as a key emphasis of tobacco control measures has been advocated, particularly in developing nations where smoking prevalence and cigarette consumption are still relatively high.
The stages of behavior change among smokers are pre-contemplation, contemplation, preparation, action, and maintenance10. Intention to quit falls in the preparation stage, which immediately precedes the action or quitting attempt stage. Smoking cessation is most effective when a spontaneous intention to quit is induced in the smoker, as evidenced in the transtheoretical model11. In a previous study, it was reported that smokers had a higher likelihood of ceasing attempts if they had smoking cessation intentions12. Therefore, recognizing characteristics connected to the desire to stop smoking is crucial for designing a successful smoking cessation approach. A study to examine the correlates of attempting to quit smoking was done based on the GATS Bangladesh 2009 data13, where intention to quit smoking has been identified14 as one of the correlates.
However, to our knowledge, limited research has examined the magnitude of intention to quit smoking and its determinants among smokers in Bangladesh15 using 2017 GATS Bangladesh data. We know that the prevalence of tobacco consumption and projected tobacco-related premature deaths are relatively high in Bangladesh. Therefore, the objective of our study was to address the prevalence and determinants of intention to quit smoking among current male smokers in Bangladesh.
METHODS
This is a secondary dataset analysis of the GATS, a cross-sectional household survey conducted among adults aged ≥15 years in 2017. All eight administrative divisions of Bangladesh were included. The detailed methodology of the survey is described elsewhere16.
Sampling design
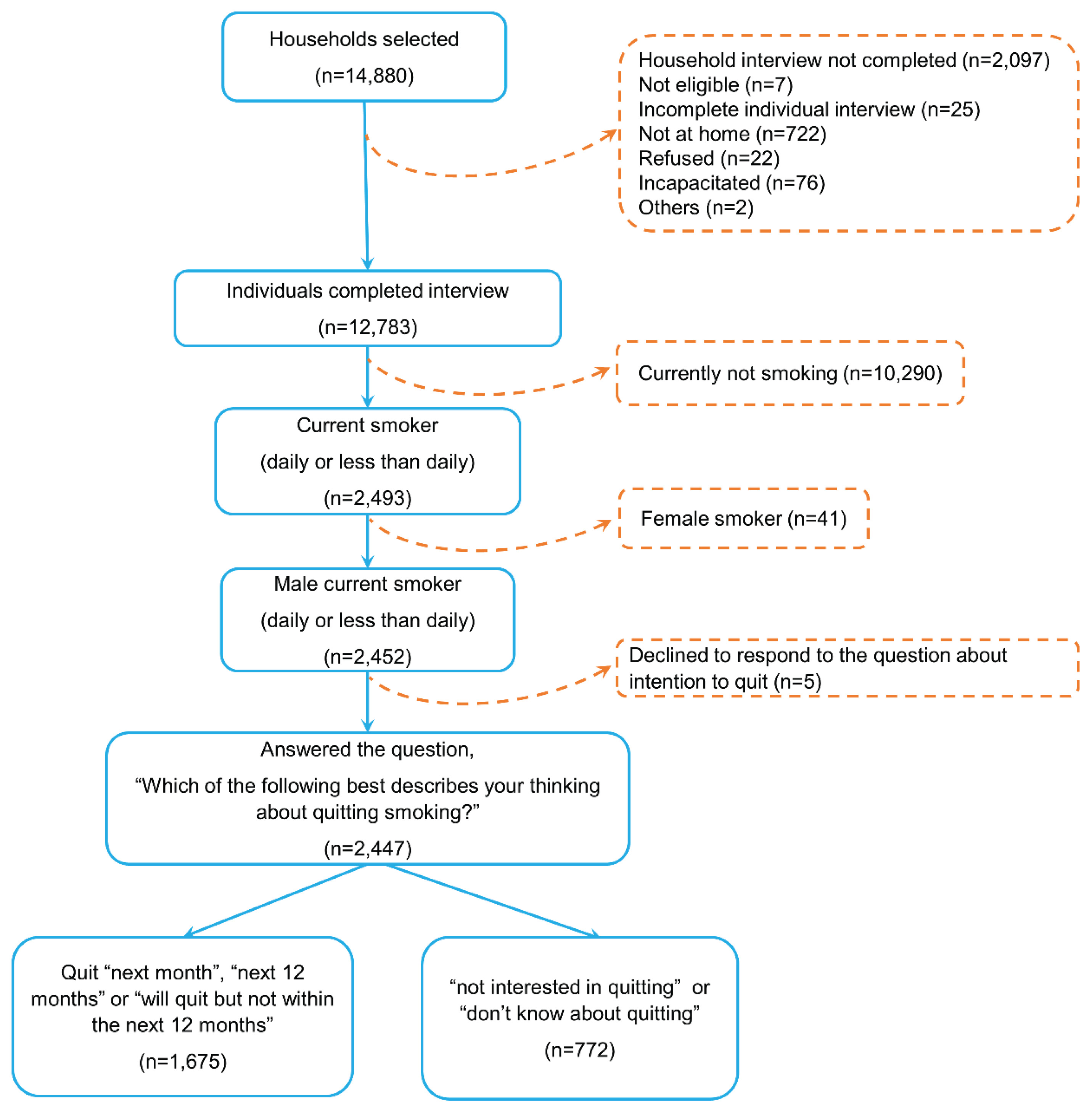
A nationally representative sample of 14880 households was selected using three-stage stratified sampling. In the first stage, 496 enumeration areas (EAs) were selected with probability proportional to the size. Among the selected EAs, 248 were urban, and 248 were rural areas. In the second stage of sampling, 30 households were selected from each EA by using systematic sampling. Finally, one individual was randomly chosen from all eligible members of a selected household. Finally, a total of 12783 respondents completed the interview, and our sample consisted of 2447 current male smokers who smoke daily or less than daily. We focused on male smokers, as there were only 33 female smokers, reflecting the very low prevalence of smoking among women in Bangladesh due to strong social and cultural norms discouraging female tobacco use (Figure 1).
Questionnaire
In GATS 2017, household and individual questionnaires were used in data collection. The individual questionnaire comprised sections on respondents’ background information, smoking, electronic cigarettes, smokeless tobacco, smoking cessation, smokeless tobacco cessation, secondary smoking, economics-tobacco, economics-bidi, economics-smokeless tobacco, media, and knowledge, attitude, practice.
Description of variables
Intention to quit
This dependent variable was created from the question: ‘Which of the following best describes your thinking about quitting smoking?’. The respondents’ answer in regard to their intention to quit smoking was divided into 4 categories: next month, next 12 months, will quit but not within the next 12 months, and not interested in quitting. Responses were dichotomized by merging the categories: next month, next 12 months, and will quit but not within the next 12 months, as having intention to quit, and those answering not interested in quitting or don’t know, as not having intention to quit. In addition, we also used this response as a continuous variable, scoring not interested in quitting as 0; will quit but not within the next 12 months as 1; next 12 months as 2; and next month as 3.
Knowledge of tobacco-related diseases
This independent variable was assessed through a set of three questions posed to respondents, inquiring whether they were aware of the connection between smoking and related diseases. Smokers who answered affirmatively to all three questions were categorized as possessing adequate knowledge regarding tobacco-related diseases, while those who did not were considered to have limited awareness of such issues.
Attempt to quit
This independent variable was assessed using the question: ‘In the last 12 months, have you made an effort to quit smoking?’. Respondents who answered ‘yes’ were categorized as individuals who had attempted to quit, while those who answered ‘no’ were regarded as individuals who had not attempted to quit.
Awareness of anti-smoking messaging
This was an independent variable assessed by a series of seven questions from the media section, each of which inquired whether the respondents saw anti-smoking materials in a specific media source (newspaper, magazine, television, radio, billboards, posters, and any specific others) over the last 30 days. Smokers who replied ‘yes’ to at least one of the seven questions were regarded as having awareness of anti-smoking messages, while those who answered ‘no’ or ‘don’t know’ to all seven questions were deemed as not having any awareness of anti-smoking messages.
Household smoking restrictions
This was an independent variable measured by the question: ‘Which of the following best describes the rules about smoking inside of your home?’. The response options were categorized and labeled as: ‘allowed’ for those who answered smoking is allowed inside of your home; there are no rules about smoking in your home was labeled as ‘no rules’; and not allowed but exceptions and never allowed were labeled as ‘not allowed’.
Nicotine dependence
The nicotine dependence measured by the heaviness of smoking index (HSI), is determined by combining scores of two variables: the number of cigarettes smoked per day and the time to the first cigarette after waking17. The number of cigarettes smoked per day is scored as follows: 0 for 1–10 cigarettes, 1 for 11–20 cigarettes, 2 for 21–30 cigarettes, and 3 for ≥31 cigarettes. The time to the first cigarette after waking is scored based on minutes: 3 for ≤5 minutes, 2 for 6–30 minutes, 1 for 31–60 minutes, and 0 for ≥61 minutes. The HSI is calculated by adding these two scores together and is divided into three levels: low (0–1), medium (2–4), and high (5–6).
Wealth index
A wealth index represents a comprehensive gauge of an individual’s household financial resources, encompassing assets, income, and living conditions. In this study, the wealth index was derived from GATS data using principal component analysis, primarily focusing on household assets18. It is often used as a proxy for socio-economic status in settings where direct income measures are not available or reliable. In this case, the population was scored on their wealth index, and the scores were used to divide the population into five equal groups or quintiles. The first quintile represents the poorest 20% of the population, and the fifth quintile represents the wealthiest 20% of the population.
Data compilation and weighting
The cleaned and compiled data underwent a weighting process to ensure its representation of the population of Bangladesh, aligning with the housing and population census of 2011 as reported by the Bangladesh Bureau of Statistics. Initially, the base weight was computed by taking the inverse of the selection probabilities for enumeration areas (EAs), households, genders, and individuals. The base weight was adjusted with non-response weights at these four levels. The final adjustment was made for the population of Bangladesh by using population calibration. The details of the weighting procedure are described elsewhere19.
Statistical analysis
Statistical analysis was performed based on IBM SPSS Statistics (version 26.0, RRID: SCR_019096) and R version 4.1.1. All estimates and their confidence intervals (CIs) were calculated after adjusting cluster, strata, and weight using the complex sample module of IBM SPSS and survey library package in R. ArcGIS pro (version 3.4.0) was used for division wise prevalence mapping.
In univariate analysis, Pearson’s chi-squared test and binomial logistic regression were used to analyze the associations between the intention to quit smoking and other factors. The logistic regression was carried out using svyglm function under survey library in R. The variables for analysis were selected a priori based on limitations and evidence from the existing literature to ensure relevance and scientific rigor. A backward stepwise logistic regression based on the Akaike information criterion (AIC) was applied to select the final model. The step functions with backward direction in R were used for the stepwise algorithm and calculated adjusted odds ratios and 95% CIs. A p<0.05 was considered statistically significant.
The dataset had very few missing values (<2% across variables). We therefore conducted a complete-case analysis and did not perform any imputation methods.
Post hoc power analysis was performed using the Kish’s effective sample size and the prevalence of intention to quit smoking. Minimum detectable effect sizes (MDES) and detectable odds ratios were calculated for key binary predictors and subgroup comparisons, indicating that the study had more than 80% power to detect small-to-moderate associations.
RESULTS
Background characteristics
In our sample (n=2447), almost half (50.6%) of the men were aged 15–39 years, with an average age of 41.5 years (95% CI: 41.0–42.0). Almost one-third (33.2%) had started regular smoking aged <18 years. More than three out of ten participants (34.9%) reported having no formal education. Nearly half of the respondents resided in urban areas (47.6%), and about 47.1% of study participants were involved in either agriculture/labor industry. Four in ten had tried to quit smoking tobacco at least once in the last 12 months. Around one-third (29.5%) of smokers were allowed to smoke at home. About 34.5% individuals had visited the doctors in the past 12 months. Almost nine out of ten respondents (88.4%) were aware of smoking-related diseases, and around two-thirds (63.4%) had noticed anti-smoking messages. Nearly one-fourth (21.9%) of the participants exhibited moderate to high levels of nicotine dependence. According to the wealth index, 23.1% were in the poorest quintile, and 14.3% in the richest (Table 1).
Table 1
Weighted* prevalence (percent, 95% confidence interval), and sample frequency of intention to quit among smoking males, Global Adult Tobacco Survey Bangladesh 2017
| Variables | Sample frequency n (%) | Intention to quit smoking % (95% CI) |
|---|---|---|
| Overall | 2447 (100) | 67.0 (63.6–70.2) |
| Age (years) | ||
| 15–39 | 1235 (50.5) | 63.2 (58.8–67.4) |
| ≥40 | 1212 (49.5) | 71.0 (66.7–74.9) |
| Age at daily smoking initiation (years) (N=2191)† | ||
| <18 | 728 (33.2) | 67.0 (61.3–72.3) |
| ≥18 | 1463 (66.8) | 66.0 (61.7–70.1) |
| Education level | ||
| No formal education | 855 (34.9) | 66.3 (61.6–70.8) |
| Primary or lower | 801 (32.7) | 67.2 (62.3–71.8) |
| Secondary and higher | 791 (32.3) | 67.6 (61.2–73.5) |
| Occupation | ||
| Govt./non-govt. employee | 268 (11.0) | 62.6 (51.5–72.5) |
| Business/self-employed | 777 (31.8) | 68.5 (63.0–73.6) |
| Agriculture/daily labor | 1152 (47.1) | 66.3 (62.1–70.2) |
| Other‡ | 250 (10.2) | 69.1 (59.7–77.1) |
| Residence | ||
| Urban | 1165 (47.6) | 62.9 (56.8–68.5) |
| Rural | 1282 (52.4) | 68.4 (64.3–72.2) |
| Attempt to quit in the past 12 months (N=2437)† | ||
| Yes | 1060 (43.5) | 81.9 (77.6–85.5) |
| No | 1377 (56.5) | 55.4 (50.6–60.2) |
| Smoking allowed at home (N=2438)† | ||
| Allowed | 718 (29.5) | 66.8 (61.2–71.9) |
| Not allowed | 841 (34.5) | 68.0 (61.0–74.3) |
| No rule | 879 (36.1) | 66.7 (61.5–71.6) |
| Visited doctors/healthcare center in the past 12 months (N=2435)† | ||
| Yes | 840 (34.5) | 75.2 (69.3–80.2) |
| No | 1595 (65.5) | 63.2 (59.1–67.0) |
| Knowledge of tobaccorelated diseases | ||
| Yes | 2162 (88.4) | 67.8 (64.3–71.2) |
| No | 285 (11.6) | 60.2 (52.4–67.6) |
| Awareness of antismoking messages in media | ||
| Yes | 1551 (63.4) | 71.2 (66.6–75.3) |
| No | 896 (36.6) | 60.6 (55.7–65.4) |
| Noticed health warning messages on packets | ||
| Yes | 67.2 (63.8–70.5) | |
| No | 62.7 (49.0–74.6) | |
| Heaviness of smoking index (N=2245)†§ | ||
| Low addiction | 1909 (78.1) | 71.2 (67.6–74.6) |
| Moderate addiction | 462 (18.9) | 52.1 (44.5–59.6) |
| High addiction | 74 (3.0) | 47.7 (33.6–62.1) |
| Wealth indexII | ||
| Poorest | 565 (23.1) | 67.0 (62.0–71.6) |
| Poorer | 551 (22.5) | 67.3 (61.2–72.9) |
| Middle | 533 (21.8) | 66.5 (59.7–72.6) |
| Rich | 449 (18.3) | 65.5 (57.0–73.2) |
| Richest | 349 (14.3) | 69.6 (60.0–77.8) |
Boldface results have p<0.05: the chi-squared test was used to assess the association between intention to quit smoking and explanatory variables.
* Sample weighted to the projected population of Bangladesh based on housing and population census of 2011.
‡ Other includes students, homemakers, housewives, houseworkers, retired personnel, unemployed, etc.
§ Heaviness of smoking index was calculated by summing two variables: the number of cigarettes smoked per day (0 = 1–10, 1 = 11–20, 2 = 21–30, 3 = ≥31) and the time to first cigarette after waking (3 = ≤5, 2 = 6–30, 1 = 31–60, and 0 = ≥61 minutes). Nicotine dependence is then categorized into a three-category variable: low (0–1), medium (2–4), and high (5–6) to create the heaviness of the smoking index17.
II Wealth index score was calculated by household assets using principal component analysis18. The entire population was grouped into 5 wealth quintiles based on these wealth index scores. The poorest category was formed from the first quintile (20% of the households with the lowest wealth score), and the richest category was formed from the last or fifth quintile (20% of households with the highest wealth score), and so on.
Prevalence of intention to quit
The overall prevalence of intention to quit smoking tobacco among current male smokers was 67.0% (95% CI: 63.6–70.2), and this was highest among respondents aged ≥40 years (71.0%; 95% CI: 66.7–74.9) and significantly higher than the respondents aged <40 years. Residents who lived in rural areas had a higher intention to quit smoking (68.4%; 95% CI: 64.3–72.2) compared to urban residents (62.9%; 95% CI: 56.8–68.5), although the difference was not statistically significant. The number of smokers who attempted to quit in the last 12 months was higher in the intention to quit smoking (81.9%; 95% CI: 77.6–85.5) group compared to those who did not make any attempt. Intention to quit existed more (75.2%, 95% CI: 69.3–80.2) among the male smokers who visited the healthcare centers compared to those who did not. Those who had the intention to quit higher number had low addiction (71.2%; 95% CI: 67.6–74.6) compared to moderate (52.1%; 95% CI: 44.5–59.6) and heavy addiction (47.7%; 95% CI: 33.6–62.1) of the HSI index smoking than those who were moderately addicted and heavy addicted (Table 1).
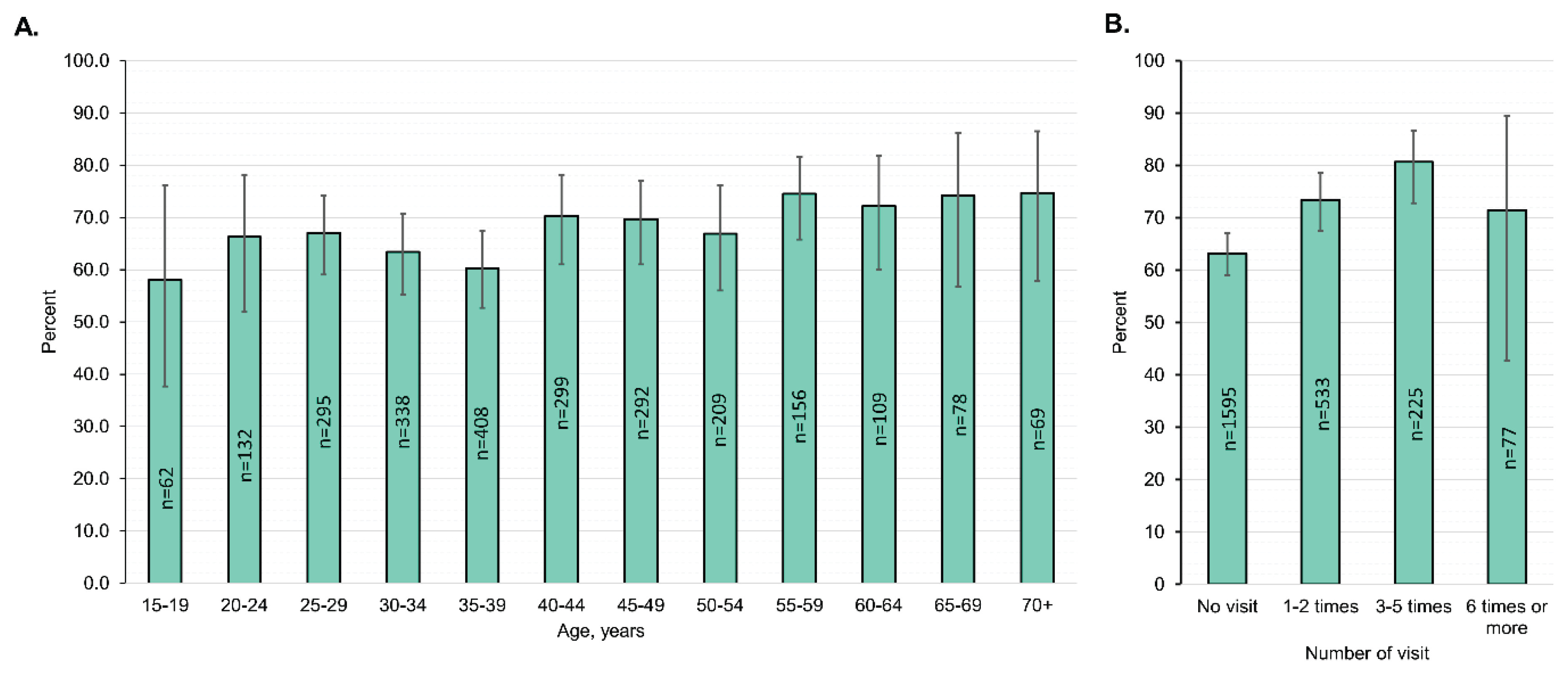
The intention to quit smoking exhibited a clear upward trend with increasing visits to doctors or healthcare centers, reaching its peak among individuals who reported up to five visits. This suggests that engagement with healthcare services may positively influence smokers’ motivation to quit. However, this trend declined among those who had six or more visits, indicating a potential plateau or even a diminishing effect of frequent healthcare interactions on quit intentions (Figure 2).
Figure 2
Weighted prevalence (%, 95% confidence interval) of intention to quit smoking among male current smokers by age (A), and number of visits to doctor or healthcare workers (B), Global Adult Tobacco Survey Bangladesh, 2017
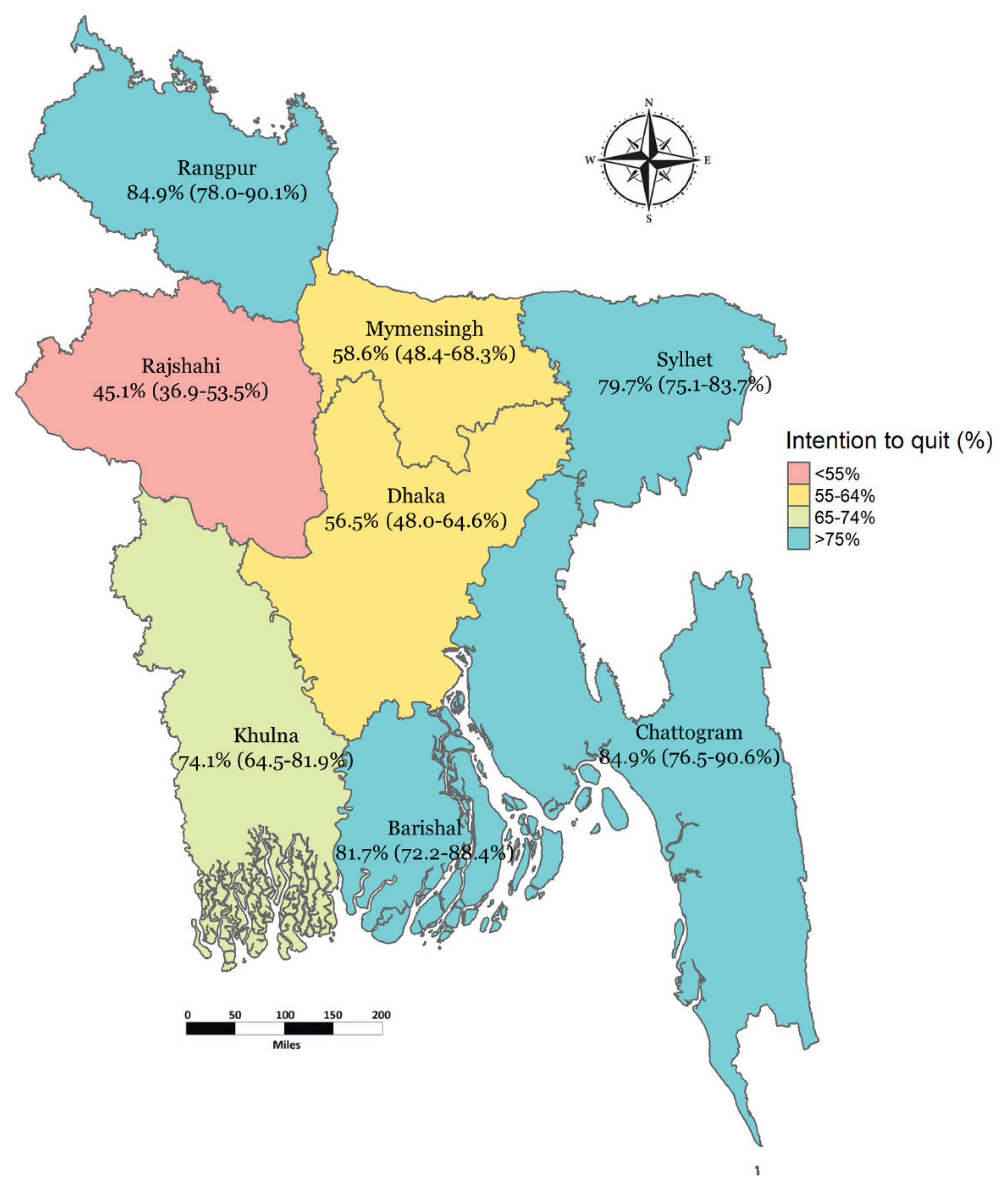
Geographically, the prevalence of intention to quit smoking was lower in the northwestern region (Rajshahi Division), followed by central areas including Dhaka and Mymensingh Divisions. In contrast, the highest levels of quit intention were observed in the southeastern region (Chattogram and Rangpur Division), followed by Barishal Divisions. These geographical patterns underscore significant regional disparities in smoking cessation motivation across Bangladesh, which may be influenced by variations in health service access, tobacco control efforts, or public awareness (Figure 3).
Factors related to the intention to quit
Multivariable logistic regression revealed that smokers aged ≥40 years had higher odds of having the intention to quit smoking compared to younger age (adjusted odds ratio, OR=1.5; 95% CI: 1.1–1.9). Smokers who attempted to quit within the past 12 months had a higher chance of intention to quit (AOR=3.2; 95% CI: 2.2–4.6) compared to those who never attempted to quit. Smokers who had noticed anti-smoking messages had significantly higher odds of intending to quit smoking (AOR=1.6; 95% CI: 1.2–2.3) compared to those who had not noticed such messages. Individuals who visited doctors or healthcare workers had higher odds of intention to quit smoking (AOR=1.6; 95% CI: 1.2–2.3). A low HSI score was more likely to be associated with an intention to quit smoking (AOR=3.1; 95% CI: 1.6–6.0) compared to heavy HSI (Table 2).
Table 2
Intention to quit smoking with different determinants among current male smokers, Global Adult Tobacco Survey Bangladesh 2017 (n=2447)
| Variables | OR (95%CI) | AOR* (95% CI) |
|---|---|---|
| Age (years) | ||
| 15–39 ® | 1 | 1 |
| ≥40 | 1.4 (1.1–1.9) | 1.5 (1.1–1.9) |
| Age at daily smoking initiation (years) (n=2191)† | ||
| <18 ® | 1 | |
| ≥18 | 1.0 (0.7–1.3) | |
| Education level | ||
| No formal education ® | 1 | |
| Primary or lower | 1.1 (0.8–1.4) | |
| Secondary and higher | 1.0 (0.7–1.5) | |
| Occupation | ||
| Govt./non-govt. employee ® | 1 | |
| Business/self-employed | 1.3 (0.7–2.2) | |
| Agriculture/daily labor | 1.3 (0.8–2.1) | |
| Other‡ | 1.5 (0.8–2.9) | |
| Residence | ||
| Urban ® | 1 | 1 |
| Rural | 1.3 (0.9–1.7) | 1.4 (0.9–2.1) |
| Attempt to quit in the past 12 months and failed (n=2437)† | ||
| No ® | 1 | 1 |
| Yes | 3.5 (2.5–5.1) | 3.2 (2.2–4.6) |
| Smoking allowed at home (n=2438)† | ||
| Allowed ® | 1 | |
| Not allowed | 1.1 (0.7–1.6) | |
| No rule | 1.0 (0.7–1.3) | |
| Visited doctors/healthcare center in the past 12 months (n=2435)† | ||
| No ® | 1 | 1 |
| Yes | 1.8 (1.2–2.5) | 1.6 (1.2–2.3) |
| Knowledge of tobaccorelated diseases | ||
| No ® | 1 | |
| Yes | 1.4 (1.0–1.9) | |
| Awareness of antismoking messages | ||
| No ® | 1 | 1 |
| Yes | 1.6 (1.2–2.2) | 1.6 (1.2–2.3) |
| Noticed health warning messages in the past 30 days | ||
| No ® | 1 | |
| Yes | 1.1 (0.5–2.1) | |
| Heaviness of smoking index (n=2445)†§ | ||
| High addiction ® | 1 | 1 |
| Moderate addiction | 1.2 (0.6–2.3) | 1.4 (0.7–2.7) |
| Low addiction | 2.6 (1.4–4.8) | 3.1 (1.6–6.0) |
| Wealth indexII | ||
| Richest ® | 1 | 1 |
| Richer | 0.8 (0.4–1.4) | 0.8 (0.4–1.5) |
| Middle | 0.9 (0.5–1.5) | 0.9 (0.5–1.7) |
| Poorer | 0.9 (0.5–1.5) | 1.1 (0.6–2.1) |
| Poorest | 0.9 (0.5–1.5) | 1.2 (0.6–2.3) |
* AOR was calculated using logistic regression to determine the factor associated with intention to quit smoking. Boldface represents statistical significance (p<0.05). A backward stepwise algorithm using Akaike information criterion (AIC) was applied in logistic regression to find the suitable model for adjusted odds ratios.
‡ Other includes students, homemakers, housewives, houseworkers, retired personnel, unemployed, etc.
§ Heaviness of smoking index was calculated by summing two variables: the number of cigarettes smoked per day (0 = 1–10, 1 = 11–20, 2 = 21–30, 3 = ≥31) and the time to first cigarette after waking (3 = ≤5, 2 = 6–30, 1 = 31–60, and 0 = ≥61 minutes). Nicotine dependence is then categorized into a three-category variable: low (0–1), medium (2–4), and high (5–6) to create the heaviness of the smoking index17.
II Wealth index score was calculated by household assets using principal component analysis18. The entire population was grouped into 5 wealth quintiles based on these wealth index scores. The poorest category was formed from the first quintile (20% of the households with the lowest wealth score), and the richest category was formed from the last or fifth quintile (20% of households with the highest wealth score), and so on. ® Reference categories.
DISCUSSION
We attempted to determine the prevalence and characteristics related to the intention to quit smoking among male smokers aged ≥15 years using nationally representative data from Bangladesh. More than two-thirds of the participants (67.0%) intended to quit smoking, with approximately one-third planning to do so within the following year.
The intention to quit smoking is high compared to a previous Bangladeshi study15, and for other Asian countries such as India (50%)20, China (23.6%)21, Malaysia (57.8%)21, and Thailand (40.2%)22. The increase in intention to quit smoking among the current male smokers might be attributed to Bangladesh’s primary tobacco control law Smoking and Use of Tobacco Products (Control) Act, 2005. Since the adoption of this law many tobacco control initiatives have been implemented in Bangladesh as a smoking-prohibited zone (public place and workplace), restrictions on tobacco advertisement, health warnings both written and graphic on the front and back of the package, prohibition of free and discounted tobacco products, and promotion of tobacco control message in different media.
However, the percentage of the intention to quit smoking in Bangladesh is similar to the United Kingdom (64.7%)23, South Korea (66.4%)24 and lower than other developed countries such as the USA (70.0%)25. This intercountry variation may be explained by the fact that each country has its own tobacco control policy. The disparity can also be attributed to methodological differences, particularly in defining the timeframe for willingness to stop; some studies operationally defined willingness to quit as ‘during the next six months’, while others defined it as ‘at any time’.
The prevalence of intention to quit smoking varied considerably across divisions. Among all the divisions, the highest rate of prevalence was observed in Rangpur and Chattogram. This finding could also be explained by a nuanced combination of socioeconomic factors, environmental challenges, levels of health awareness, and evolving cultural perspectives. Also, the regional tobacco control efforts could be unevenly effective. Bangladesh’s Tobacco Control Act and the WHO Framework Convention commitments have rolled out policies like taxes and warnings, but enforcement and awareness vary. Rangpur’s proximity to tobacco production might mean more targeted interventions, while Chattogram’s urban centers could see stronger public health campaigns. Workplace smoking policies or home smoking rules, which influence quit intentions, might also differ in impact here. This also might be attributed to a complex interplay of socioeconomic pressures, environmental degradation, health awareness, and shifting cultural attitudes15.
In our sample, those who were aged ≥40 years, resided in rural areas, attempted to quit in the last 12 months, visited doctors/healthcare centers, noticed anti-smoking messages on billboards/hoardings, and had low addiction to smoking, had the intention to quit. Our findings about older age being associated with significantly higher odds of intention to quit smoking are consistent with previous research26. However, few studies reported that older age has lower odds of intention to quit than younger age24,27, and others conveyed no association15. The differences in quitting intention among different age groups may be explained by the percentage of vulnerability to health due to smoking. Since older people are more vulnerable to the health impacts of smoking, and thus, in our study, older people were more likely to have the intention to quit smoking28.
We did not find any significant difference in intention to quit smoking among different levels of education. One study in the Netherlands reported no educational differences in the intention to quit29. On the contrary, few studies reported that more highly educated people were more likely to have an intention of quitting23. In our study, we observed almost constant intention to quit smoking among different wealth quintiles. Contradictorily, several studies have found that high-income individuals have a higher intention to quit smoking than low-income individuals30. Also, a study in Nigeria reported that respondents with primary education were nearly three times more likely to have the intention to quit than tertiary education31. Moreover, the relationship between sociodemographic factors and smoking cessation is not always stable.
Having a history of past quitting attempts was positively associated with intention to quit smoking compared to having no attempt. This is in line with a study in China21. These findings are most likely the result of variations in smokers’ readiness to stop smoking, as smokers who have already failed to stop smoking earlier may maintain a strong intention to do so, whereas smokers who have never tried to stop smoking may simply not be prepared to stop and have no intention to do so. This implies the need to encourage smokers to consider quitting by focusing on awareness of the benefits of quitting.
Our study showed that the intention to smoke cessation was higher among the participants who visited doctors or healthcare centers at least once in the last 12 months. Other studies reported that 3- to 8-day residential programs intervening in professional counseling and medication treatment are effective in smoking cessation32. Another quasi-experimental study in Taiwan showed that advice from physicians and nurses enhanced the force towards smoking cessation, but only for those who had ever considered quitting and intended to do so in the following month or next six months, and not significant for those who had never attempted any quitting33. Our study suggests that increasing the number of doctor visits increases the proportion of intention to quit smoking up to five visits and starts to decline for six or more visits. This may be because individuals who visit the doctor more frequently are more likely to have higher motivation to quit smoking and may be more receptive to smoking cessation interventions. However, there might be a message fatigue34 at play for our sample, which is reflected by the decline of participants having the intention to quit for six or more visits.
Anti-smoking mass media campaigns facilitate cutting back the prevalence of smoking by encouraging current smokers to quit through awareness building. Effective anti-smoking messages shown in movie theaters raise knowledge of the negative effects of smoking and have been demonstrated to boost smokers’ intentions to give up35. In line with this, our study also revealed that individuals who noticed any anti-smoking message were more likely to intend to quit smoking.
Heavy nicotine dependence is a major obstacle to quitting smoking and quitting efforts36. Smokers who are less dependent on nicotine are thought to stop smoking more frequently, leaving a smaller percentage of extremely dependent (also known as ‘hardcore’) smokers in the community. In our study, smokers who had low HSI scores were more likely to have the intention to quit compared to their counterparts. These results suggest that cessation strategies should be tuned to the smoker’s intensity of nicotine dependence. Smokers with lower dependence should be encouraged to quit smoking.
Strengths and limitations
This study presents the results of an analysis of nationally representative data and the inclusion of known standardized measures associated with the intention to quit smoking collected through a globally standardized GATS Protocol13 in Bangladeshi adults. Regardless of the strength, the study has some limitations. First, the cross-sectional design precludes causal inference between the identified factors and the intention to quit smoking. Second, although we adjusted for a range of covariates, the possibility of residual confounding due to unmeasured or inadequately measured variables (e.g. access to cessation services, alcohol consumption, or psychosocial factors) cannot be ruled out. Third, as the data were collected through interviewer-administered surveys, social desirability and response biases may have influenced participants’ answers. Finally, while the use of a nationally representative sample strengthens the relevance of our findings for Bangladesh, the generalizability to other countries or cultural contexts may be limited.
CONCLUSIONS
A large proportion of adult smokers in Bangladesh expressed a desire to quit smoking. Enhancing intention to quit rates among tobacco users, especially those with lower addiction rates and prior stop attempts, may be achieved by implementing stricter rules and offering concise counseling from physicians during encounters. Furthermore, the research highlights the efficacy of using billboards or hoardings, including anti-tobacco messaging, as a helpful intervention tool for smokers. This study may inspire the development of a national strategic plan to integrate the evidence and formulate programs to facilitate the growing demand to quit smoking.